

Statins and All-Cause Mortality in Patients Undergoing Hemodialysis
- PMID: 32089045
- PMCID: PMC7335561
- DOI: 10.1161/JAHA.119.014840
Statins and All-Cause Mortality in Patients Undergoing Hemodialysis
Abstract
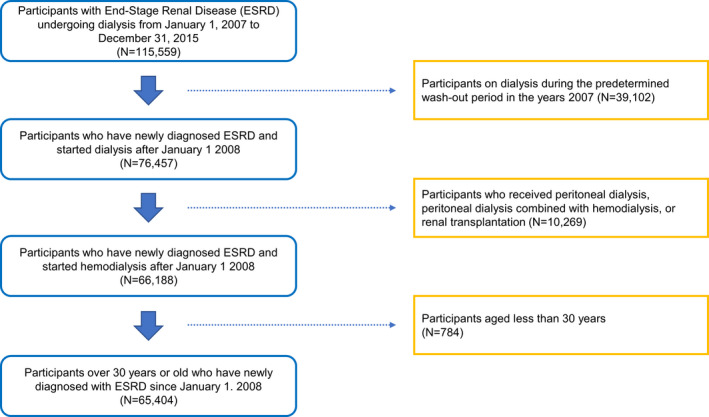
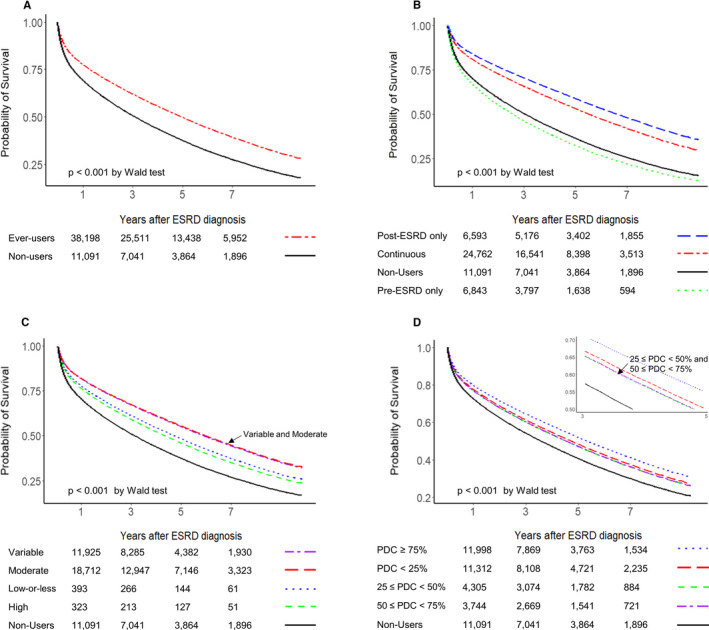
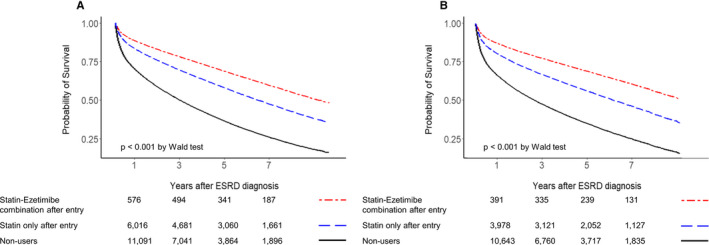
Background Recommendations have not yet been established for statin therapy in patients on maintenance dialysis. In this study, we aimed to evaluate the effects of statin therapy on all-cause mortality in patients undergoing maintenance hemodialysis. Methods and Results This retrospective cohort study analyzed data from adults, aged ≥30 years, who were on maintenance hemodialysis for end-stage renal disease. Data on statin use, along with other clinical information between 2007 and 2017, were extracted from the Health Insurance Review and Assessment Service database in Korea. In total, 65 404 patients were included, and 41 549 (73.2%) patients had received statin therapy for a mean duration of 3.6±2.6 years. Compared with statin nonusers before and after the initiation of hemodialysis (entry), patients who initiated statin therapy after entry and patients who continued statins from the pre-end-stage renal disease to post-end-stage renal disease period had a lower risk of all-cause mortality; the adjusted hazard ratios (95% CIs) were 0.48 (0.47-0.50; P<0.001) for post-end-stage renal disease only statin users and 0.59 (0.57-0.60; P<0.001) for continuous statin users. However, those discontinuing statins before or at entry showed a higher risk of all-cause mortality. Statin-ezetimibe combinations were associated with better survival benefits than fixed patterns of statin therapy. These results were consistent across various subgroups, including elderly patients aged >75 years, and were maintained even after propensity score matching. Conclusions Our results showed that in adult patients undergoing maintenance hemodialysis, statin therapy, preferably combined with ezetimibe, was associated with a lower risk of all-cause mortality.
Keywords: all‐cause mortality; end‐stage renal diseases; hemodialysis; statin.
Figures
Similar articles
-
Statin Therapy Before Transition to End-Stage Renal Disease With Posttransition Outcomes.J Am Heart Assoc. 2019 Mar 19;8(6):e011869. doi: 10.1161/JAHA.118.011869. J Am Heart Assoc. 2019. PMID: 30885048 Free PMC article.
-
Moderate to high intensity statin in dialysis patients after acute myocardial infarction: A national cohort study in Asia.Atherosclerosis. 2017 Dec;267:158-166. doi: 10.1016/j.atherosclerosis.2017.09.018. Epub 2017 Sep 27. Atherosclerosis. 2017. PMID: 28985950
-
Statin initiation and all-cause mortality in incident statin-naïve dialysis patients.Atherosclerosis. 2021 Nov;337:59-65. doi: 10.1016/j.atherosclerosis.2021.08.026. Epub 2021 Aug 17. Atherosclerosis. 2021. PMID: 34429195
-
Precision Medicine and Personalized Management of Lipoprotein and Lipid Disorders in Chronic and End-Stage Kidney Disease.Semin Nephrol. 2018 Jul;38(4):369-382. doi: 10.1016/j.semnephrol.2018.05.007. Semin Nephrol. 2018. PMID: 30082057 Review.
-
Safety and efficacy of statins in patients with end-stage renal disease.Ann Pharmacother. 2013 Oct;47(10):1321-9. doi: 10.1177/1060028013501997. Epub 2013 Oct 17. Ann Pharmacother. 2013. PMID: 24259696 Review.
Cited by
-
Alirocumab and Lipid Levels, Inflammatory Biomarkers, Metabolomics, and Safety in Patients Receiving Maintenance Dialysis: The ALIrocumab in DIALysis Study (A Phase 3 Trial to Evaluate the Efficacy and Safety of Biweekly Alirocumab in Patients on a Stable Dialysis Regimen).Kidney Med. 2022 May 20;4(7):100483. doi: 10.1016/j.xkme.2022.100483. eCollection 2022 Jul. Kidney Med. 2022. PMID: 35801187 Free PMC article.
-
Associations Between Low-Density Lipoprotein Cholesterol Levels and Cardiovascular Outcomes in Patients Undergoing Dialysis: A Nationwide Cohort Study.J Clin Med. 2025 Jul 8;14(14):4845. doi: 10.3390/jcm14144845. J Clin Med. 2025. PMID: 40725536 Free PMC article.
-
Managing dyslipidaemia in patients with chronic kidney disease.Indian Heart J. 2024 Mar;76 Suppl 1(Suppl 1):S90-S92. doi: 10.1016/j.ihj.2024.01.012. Epub 2024 Jan 24. Indian Heart J. 2024. PMID: 38278323 Free PMC article. Review.
-
The Protective Effects of Lipid-Lowering Agents on Cardiovascular Disease and Mortality in Maintenance Dialysis Patients: Propensity Score Analysis of a Population-Based Cohort Study.Front Pharmacol. 2022 Jan 28;12:804000. doi: 10.3389/fphar.2021.804000. eCollection 2021. Front Pharmacol. 2022. PMID: 35153758 Free PMC article.
-
The Effect of Statins in Cancer Risk Reduction in Patients on Dialysis: A Population-Based Case-Control Study.J Clin Med. 2021 Nov 28;10(23):5602. doi: 10.3390/jcm10235602. J Clin Med. 2021. PMID: 34884304 Free PMC article.
References
-
- Chou R, Dana T, Blazina I, Daeges M, Jeanne TL. Statins for prevention of cardiovascular disease in adults: evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2016;316:2008–2024. - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, Braun LT, de Ferranti S, Faiella‐Tommasino J, Forman DE, Goldberg R, Heidenreich PA, Hlatky MA, Jones DW, Lloyd‐Jones D, Lopez‐Pajares N, Ndumele CE, Orringer CE, Peralta CA, Saseen JJ, Smith SC Jr, Sperling L, Virani SS, Yeboah J. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139:e1082–e1143. - PMC - PubMed
-
- Wanner C, Tonelli M. KDIGO Clinical Practice Guideline for Lipid Management in CKD: summary of recommendation statements and clinical approach to the patient. Kidney Int. 2014;85:1303–1309. - PubMed
-
- Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, Chapman MJ, De Backer GG, Delgado V, Ference BA, Graham IM, Halliday A, Landmesser U, Mihaylova B, Pedersen TR, Riccardi G, Richter DJ, Sabatine MS, Taskinen MR, Tokgozoglu L, Wiklund O. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41:111–118. - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd‐Jones DM, McBride P, Schwartz JS, Shero ST, Smith SC Jr, Watson K, Wilson PW, Eddleman KM, Jarrett NM, LaBresh K, Nevo L, Wnek J, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, DeMets D, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Smith SC Jr, Tomaselli GF. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S1–S45. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
