

Electrophysiology Testing to Stratify Patients With Left Bundle Branch Block After Transcatheter Aortic Valve Implantation
- PMID: 32089049
- PMCID: PMC7335581
- DOI: 10.1161/JAHA.119.014446
Electrophysiology Testing to Stratify Patients With Left Bundle Branch Block After Transcatheter Aortic Valve Implantation
Abstract
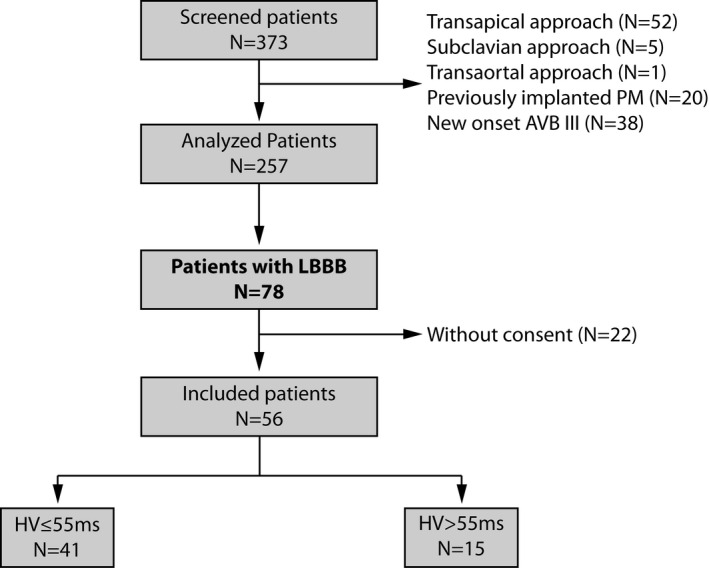
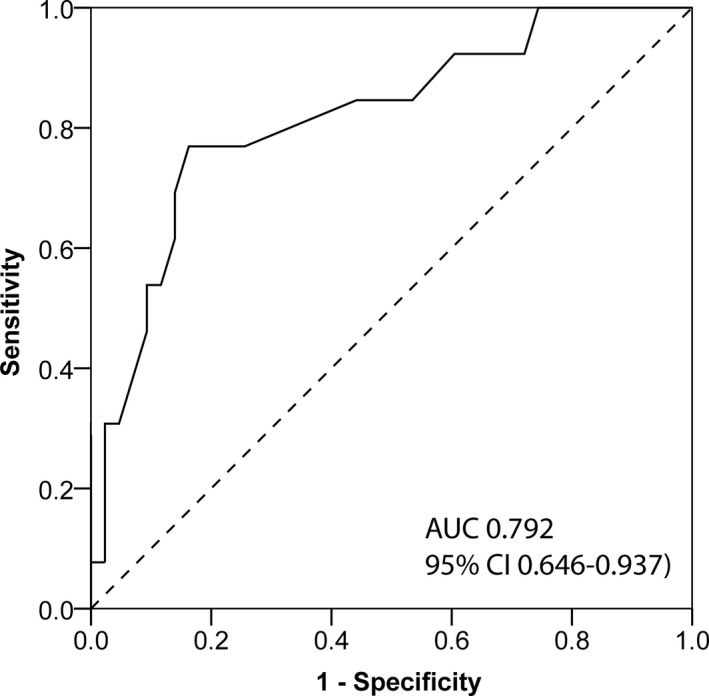
Background Left bundle branch block (LBBB) is common after transcatheter aortic valve implantation (TAVI) and is an indicator of subsequent high-grade atrioventricular block (HAVB). No standardized protocol is available to identify LBBB patients at risk for HAVB. The aim of the current study was to evaluate the safety and efficacy of an electrophysiology study tailored strategy in patients with LBBB after TAVI. Methods and Results We prospectively analyzed consecutive patients with LBBB after TAVI. An electrophysiology study was performed to measure the HV-interval the day following TAVI. In patients with normal His-ventricular (HV)-interval ≤55 ms, a loop recorder was implanted (ILR-group), whereas pacemaker implantation was performed in patients with prolonged HV-interval >55 ms (PM-group). The primary end point was occurrence of HAVB during a follow-up of 12 months. Secondary end points were symptoms, hospitalizations, adverse events because of device implantation or electrophysiology study, and death. Of 373 patients screened after TAVI, 56 patients (82±6 years, 41% male) with LBBB were included. HAVB occurred in 4 of 41 patients (10%) in the ILR-group and in 8 of 15 patients (53%) in the PM-group (P<0.001). We did not identify other predictors for HAVB than the HV interval. The negative predictive value for the cut-off of HV 55 ms to detect HAVB was 90%. No HAVB-related syncope occurred in the 2 groups. Conclusions An electrophysiology study tailored strategy to LBBB after TAVI with a cut-off of HV >55 ms is a feasible and safe approach to stratify patients with regard to developing HAVB during a follow-up of 12 months.
Keywords: electrophysiology study; high‐grade AV block; left bundle branch block; transaortic valve implantation.
Figures
Similar articles
-
Incidence and management of atrioventricular conduction disorders in new-onset left bundle branch block after TAVI: A prospective multicenter study.Heart Rhythm. 2023 May;20(5):699-706. doi: 10.1016/j.hrthm.2023.01.013. Epub 2023 Jan 13. Heart Rhythm. 2023. PMID: 36646235
-
Arrhythmic Burden as Determined by Ambulatory Continuous Cardiac Monitoring in Patients With New-Onset Persistent Left Bundle Branch Block Following Transcatheter Aortic Valve Replacement: The MARE Study.JACC Cardiovasc Interv. 2018 Aug 13;11(15):1495-1505. doi: 10.1016/j.jcin.2018.04.016. Epub 2018 Jul 18. JACC Cardiovasc Interv. 2018. PMID: 30031719
-
Early Resolution of New-Onset Left Bundle Branch Block After Transcatheter Aortic Valve Implantation With the SAPIEN 3 Valve.Am J Cardiol. 2022 Apr 1;168:117-127. doi: 10.1016/j.amjcard.2021.12.032. Epub 2022 Jan 16. Am J Cardiol. 2022. PMID: 35045936
-
Role of Routine Electrophysiological Study Performed During Transcatheter Aortic Valve Replacement to Predict AV Block.Pacing Clin Electrophysiol. 2025 Apr;48(4):377-385. doi: 10.1111/pace.15159. Epub 2025 Feb 6. Pacing Clin Electrophysiol. 2025. PMID: 39913105 Review.
-
[Transcatheter aortic valve implantation and conduction disturbances].Ann Cardiol Angeiol (Paris). 2019 Dec;68(6):443-449. doi: 10.1016/j.ancard.2019.09.024. Epub 2019 Oct 23. Ann Cardiol Angeiol (Paris). 2019. PMID: 31668339 Review. French.
Cited by
-
[[Results after implementation of the European protocol in the management of post-TAVI conduction disorders]].REC Interv Cardiol. 2025 Feb 6;7(2):122-124. doi: 10.24875/RECIC.M24000499. eCollection 2025 Apr-Jun. REC Interv Cardiol. 2025. PMID: 40438643 Free PMC article. Spanish. No abstract available.
-
Advantages and disadvantages of drug challenge during electrophysiological study in patients with new left bundle branch block after transaortic valve implantation.Int J Cardiol Heart Vasc. 2022 Jan 28;39:100961. doi: 10.1016/j.ijcha.2022.100961. eCollection 2022 Apr. Int J Cardiol Heart Vasc. 2022. PMID: 35155737 Free PMC article.
-
Role of cardiac event monitor in the detection of delayed high-grade atrioventricular block after negative electrophysiological study in patients with post-transcatheter aortic valve replacement.Heart Rhythm O2. 2024 Jul 5;5(8):587-591. doi: 10.1016/j.hroo.2024.07.002. eCollection 2024 Aug. Heart Rhythm O2. 2024. PMID: 39263618 Free PMC article. No abstract available.
-
Value of Periprocedural Electrophysiology Testing During Transcatheter Aortic Valve Replacement for Risk Stratification of Patients With New-Onset Left Bundle-Branch Block.J Am Heart Assoc. 2022 Aug 2;11(15):e026239. doi: 10.1161/JAHA.122.026239. Epub 2022 Jul 25. J Am Heart Assoc. 2022. PMID: 35876404 Free PMC article.
-
Reducing CIED-Related Morbidity: "LESS Is More".J Clin Med. 2022 Aug 16;11(16):4782. doi: 10.3390/jcm11164782. J Clin Med. 2022. PMID: 36013022 Free PMC article.
References
-
- Himbert D, Descoutures F, Al‐Attar N, Iung B, Ducrocq G, Detaint D, Brochet E, Messika‐Zeitoun D, Francis F, Ibrahim H, Nataf P, Vahanian A. Results of transfemoral or transapical aortic valve implantation following a uniform assessment in high‐risk patients with aortic stenosis. J Am Coll Cardiol. 2009;54:303–311. - PubMed
-
- Cribier A, Eltchaninoff H, Tron C, Bauer F, Agatiello C, Nercolini D, Tapiero S, Litzler PY, Bessou JP, Babaliaros V. Treatment of calcific aortic stenosis with the percutaneous heart valve: mid‐term follow‐up from the initial feasibility studies: the French experience. J Am Coll Cardiol. 2006;47:1214–1223. - PubMed
-
- Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria JE, Herrmann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S. Transcatheter aortic‐valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–1607. - PubMed
-
- Brignole M, Auricchio A, Baron‐Esquivias G, Bordachar P, Boriani G, Breithardt OA, Cleland J, Deharo JC, Delgado V, Elliott PM, Gorenek B, Israel CW, Leclercq C, Linde C, Mont L, Padeletti L, Sutton R, Vardas PE, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S, Kirchhof P, Blomstrom‐Lundqvist C, Badano LP, Aliyev F, Bansch D, Baumgartner H, Bsata W, Buser P, Charron P, Daubert JC, Dobreanu D, Faerestrand S, Hasdai D, Hoes AW, Le Heuzey JY, Mavrakis H, McDonagh T, Merino JL, Nawar MM, Nielsen JC, Pieske B, Poposka L, Ruschitzka F, Tendera M, Van Gelder IC, Wilson CM. 2013 ESC guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J. 2013;34:2281–2329. - PubMed
-
- Franzoni I, Latib A, Maisano F, Costopoulos C, Testa L, Figini F, Giannini F, Basavarajaiah S, Mussardo M, Slavich M, Taramasso M, Cioni M, Longoni M, Ferrarello S, Radinovic A, Sala S, Ajello S, Sticchi A, Giglio M, Agricola E, Chieffo A, Montorfano M, Alfieri O, Colombo A. Comparison of incidence and predictors of left bundle branch block after transcatheter aortic valve implantation using the CoreValve versus the Edwards valve. Am J Cardiol. 2013;112:554–559. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
