

Endoscopic Kyoto classification of Helicobacter pylori infection and gastric cancer risk diagnosis
- PMID: 32089624
- PMCID: PMC7015719
- DOI: 10.3748/wjg.v26.i5.466
Endoscopic Kyoto classification of Helicobacter pylori infection and gastric cancer risk diagnosis
Abstract
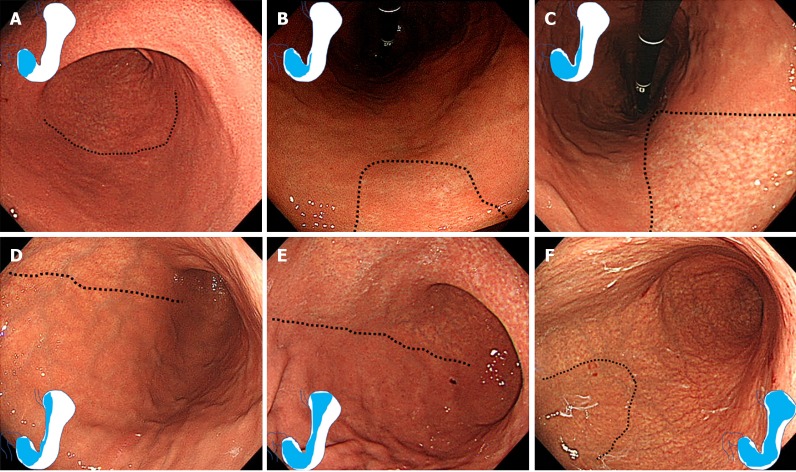
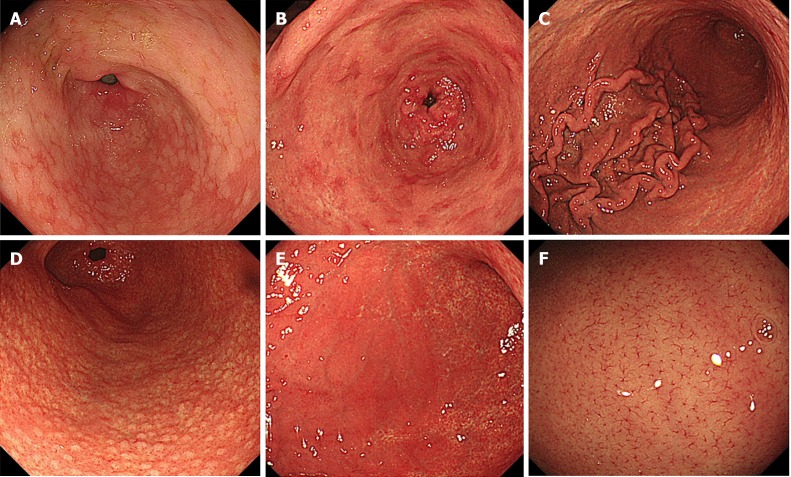
Recent advances in endoscopic technology allow detailed observation of the gastric mucosa. Today, endoscopy is used in the diagnosis of gastritis to determine the presence/absence of Helicobacter pylori (H. pylori) infection and evaluate gastric cancer risk. In 2013, the Japan Gastroenterological Endoscopy Society advocated the Kyoto classification, a new grading system for endoscopic gastritis. The Kyoto classification organized endoscopic findings related to H. pylori infection. The Kyoto classification score is the sum of scores for five endoscopic findings (atrophy, intestinal metaplasia, enlarged folds, nodularity, and diffuse redness with or without regular arrangement of collecting venules) and ranges from 0 to 8. Atrophy, intestinal metaplasia, enlarged folds, and nodularity contribute to gastric cancer risk. Diffuse redness and regular arrangement of collecting venules are related to H. pylori infection status. In subjects without a history of H. pylori eradication, the infection rates in those with Kyoto scores of 0, 1, and ≥ 2 were 1.5%, 45%, and 82%, respectively. A Kyoto classification score of 0 indicates no H. pylori infection. A Kyoto classification score of 2 or more indicates H. pylori infection. Kyoto classification scores of patients with and without gastric cancer were 4.8 and 3.8, respectively. A Kyoto classification score of 4 or more might indicate gastric cancer risk.
Keywords: Atrophy; Diffuse redness; Endoscopy; Enlarged fold; Gastric cancer; Helicobacter pylori; Intestinal metaplasia; Kyoto classification; Nodularity; Regular arrangement of collecting venules.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: Authors declare no conflict of interests for this article.
Figures
References
-
- Draganov PV, Wang AY, Othman MO, Fukami N. AGA Institute Clinical Practice Update: Endoscopic Submucosal Dissection in the United States. Clin Gastroenterol Hepatol. 2019;17:16–25.e1. - PubMed
-
- Malfertheiner P, Megraud F, O'Morain CA, Gisbert JP, Kuipers EJ, Axon AT, Bazzoli F, Gasbarrini A, Atherton J, Graham DY, Hunt R, Moayyedi P, Rokkas T, Rugge M, Selgrad M, Suerbaum S, Sugano K, El-Omar EM European Helicobacter and Microbiota Study Group and Consensus panel. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut. 2017;66:6–30. - PubMed
-
- Sakitani K, Nishizawa T, Arita M, Yoshida S, Kataoka Y, Ohki D, Yamashita H, Isomura Y, Toyoshima A, Watanabe H, Iizuka T, Saito Y, Fujisaki J, Yahagi N, Koike K, Toyoshima O. Early detection of gastric cancer after Helicobacter pylori eradication due to endoscopic surveillance. Helicobacter. 2018;23:e12503. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
