

Artificial intelligence in medical imaging: A radiomic guide to precision phenotyping of cardiovascular disease
- PMID: 32090243
- PMCID: PMC7585409
- DOI: 10.1093/cvr/cvaa021
Artificial intelligence in medical imaging: A radiomic guide to precision phenotyping of cardiovascular disease
Abstract
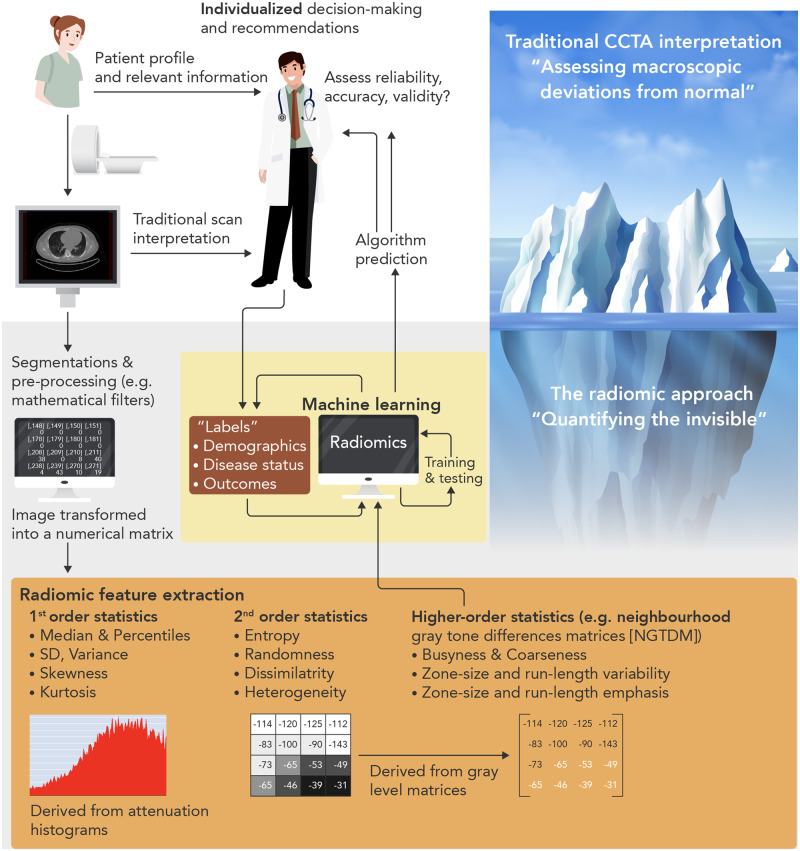
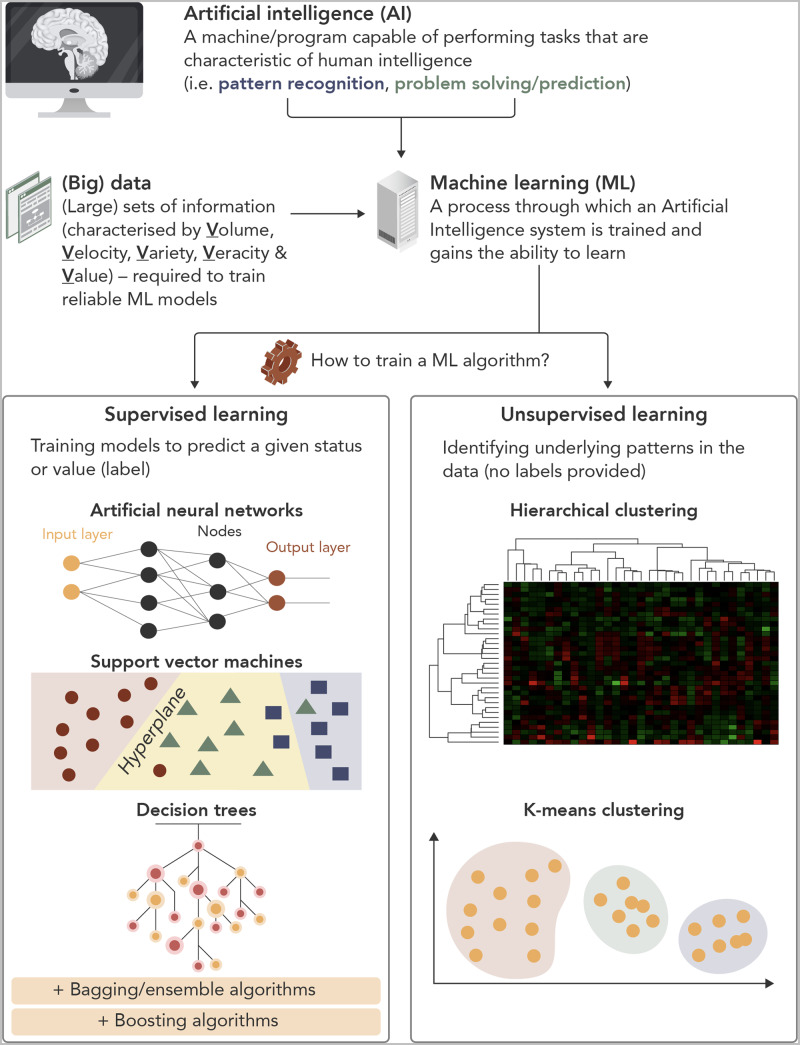
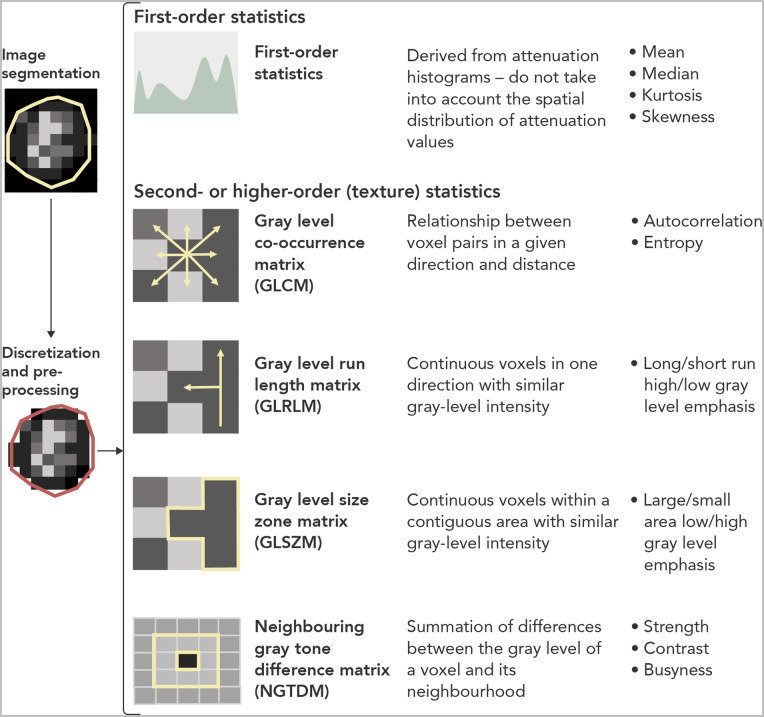
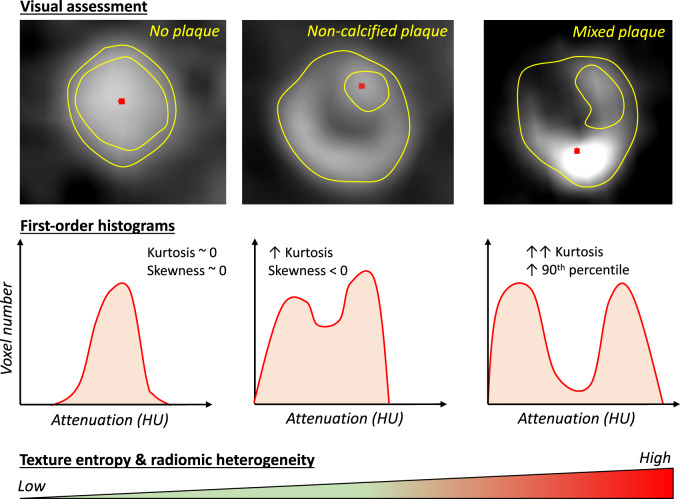
Rapid technological advances in non-invasive imaging, coupled with the availability of large data sets and the expansion of computational models and power, have revolutionized the role of imaging in medicine. Non-invasive imaging is the pillar of modern cardiovascular diagnostics, with modalities such as cardiac computed tomography (CT) now recognized as first-line options for cardiovascular risk stratification and the assessment of stable or even unstable patients. To date, cardiovascular imaging has lagged behind other fields, such as oncology, in the clinical translational of artificial intelligence (AI)-based approaches. We hereby review the current status of AI in non-invasive cardiovascular imaging, using cardiac CT as a running example of how novel machine learning (ML)-based radiomic approaches can improve clinical care. The integration of ML, deep learning, and radiomic methods has revealed direct links between tissue imaging phenotyping and tissue biology, with important clinical implications. More specifically, we discuss the current evidence, strengths, limitations, and future directions for AI in cardiac imaging and CT, as well as lessons that can be learned from other areas. Finally, we propose a scientific framework in order to ensure the clinical and scientific validity of future studies in this novel, yet highly promising field. Still in its infancy, AI-based cardiovascular imaging has a lot to offer to both the patients and their doctors as it catalyzes the transition towards a more precise phenotyping of cardiovascular disease.
Keywords: Artificial intelligence; Atherosclerosis; Computed tomography; Plaque; Radiomics; Risk prediction.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med 2019;25:44–56. - PubMed
-
- National Institute for Health and Care Excellence (NICE). Chest pain of recent onset: assessment and diagnosis. Clinical Guideline [CG95]. https://www.nice.org.uk/guidance/cg95?unlid=28903932120171912336 (date last accessed 27 July 2019). - PubMed
-
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, Agewall S, Dickstein K, Edvardsen T, Escaned J, Gersh BJ, Svitil P, Gilard M, Hasdai D, Hatala R, Mahfoud F, Masip J, Muneretto C, Valgimigli M, Achenbach S, Bax JJ; ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 2020;41:407–477. - PubMed
-
- Task Force MembersMontalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Budaj A, Bugiardini R, Crea F, Cuisset T, Di Mario C, Ferreira JR, Gersh BJ, Gitt AK, Hulot JS, Marx N, Opie LH, Pfisterer M, Prescott E, Ruschitzka F, Sabaté M, Senior R, Taggart DP, van der Wall EE, Vrints CJESC Committee for Practice GuidelinesZamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker SDocument ReviewersKnuuti J, Valgimigli M, Bueno H, Claeys MJ, Donner-Banzhoff N, Erol C, Frank H, Funck-Brentano C, Gaemperli O, Gonzalez-Juanatey JR, Hamilos M, Hasdai D, Husted S, James SK, Kervinen K, Kolh P, Kristensen SD, Lancellotti P, Maggioni AP, Piepoli MF, Pries AR, Romeo F, Rydén L, Simoons ML, Sirnes PA, Steg PG, Timmis A, Wijns W, Windecker S, Yildirir A, Zamorano JL. 2013 ESC guidelines on the management of stable coronary artery disease: the Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J 2013;34:2949–3003. - PubMed
-
- Douglas PS, Hoffmann U, Patel MR, Mark DB, Al-Khalidi HR, Cavanaugh B, Cole J, Dolor RJ, Fordyce CB, Huang M, Khan MA, Kosinski AS, Krucoff MW, Malhotra V, Picard MH, Udelson JE, Velazquez EJ, Yow E, Cooper LS, Lee KL PROMISE Investigators. Outcomes of anatomical versus functional testing for coronary artery disease. N Engl J Med 2015;372:1291–1300. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
