

Implementation of Enhanced Recovery After Surgery (ERAS) protocol in off-pump coronary artery bypass graft surgery. A prospective cohort feasibility study
- PMID: 32090310
- PMCID: PMC10173132
- DOI: 10.5114/ait.2020.93160
Implementation of Enhanced Recovery After Surgery (ERAS) protocol in off-pump coronary artery bypass graft surgery. A prospective cohort feasibility study
Abstract
Background: Coronary artery bypass graft (CABG) is the most commonly performed cardiac surgery procedure. Although some complications related to the cardiopulmonary bypass circuit are avoided during off-pump CABG (OP-CABG) procedures, prolonged mechanical ventilation and severe postoperative pain are still important issues.
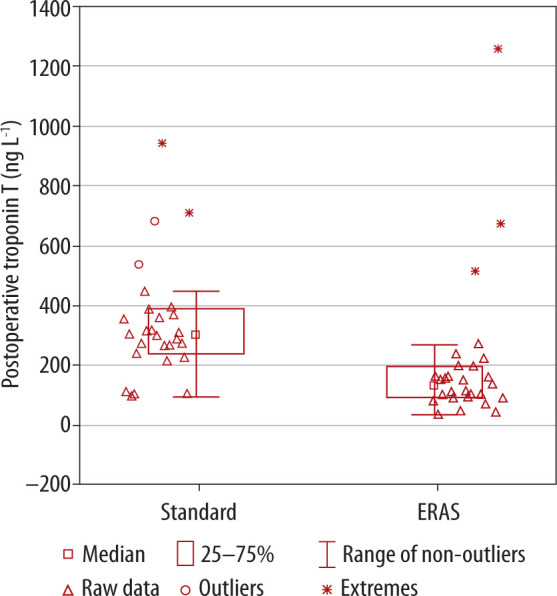
Methods: This prospective cohort study aimed to assess the impact of the institutional Enhanced Recovery After Surgery (ERAS) protocol in patients undergoing OP-CABG. This protocol contained several modifications to the perioperative period, among which bilateral erector spinae plane block, remifentanil infusion, and patient-controlled analgesia (PCA) with oxycodone were the most important factors (ERAS group). The ERAS group was compared with the retrospective cohort (same surgeon) before the ERAS protocol was implemented (standard care group). The outcomes measured included the postoperative mechanical ventilation time, ICU and hospital stay, postoperative drainage time, postoperative troponin T level, pain severity evaluated via a numerical rating scale, and the total consumption of opioids in both groups of patients.
Results: Overall, 57 patients were analyzed - 29 in the ERAS group and 28 in the standard care group. The time of mechanical ventilation, thoracic drainage, and ICU and hospital stay was shorter in the ERAS group than in the standard care group. The pain was less intense in the ERAS patients, and the postoperative opioid demand was reduced. Moreover, the increase of the postoperative troponin T concentration was lower in the ERAS group.
Conclusions: Our study showed that ERAS protocol implementation could improve patient outcomes after OP-CABG surgery.
Keywords: Enhanced Recovery After Surgery; coronary artery bypass graft; erector spinae plane block; numerical rating scale; patient-controlled analgesia.
Conflict of interest statement
none.
Figures
References
-
- Weiss AJ, Elixhauser A. Trends in Operating Room Procedures in U.S. Hospitals, 2001-2011: Statistical Brief #171. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD): Agency for Healthcare Research and Quality (US), 2006. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous