

Percutaneous Radiofrequency Ablation for Metachronous Hepatic Metastases after Curative Resection of Pancreatic Adenocarcinoma
- PMID: 32090524
- PMCID: PMC7039725
- DOI: 10.3348/kjr.2019.0647
Percutaneous Radiofrequency Ablation for Metachronous Hepatic Metastases after Curative Resection of Pancreatic Adenocarcinoma
Abstract
Objective: To retrospectively evaluate the safety and efficacy of percutaneous radiofrequency ablation (RFA) in patients with metachronous hepatic metastases arising from pancreatic adenocarcinoma who had previously received curative surgery.
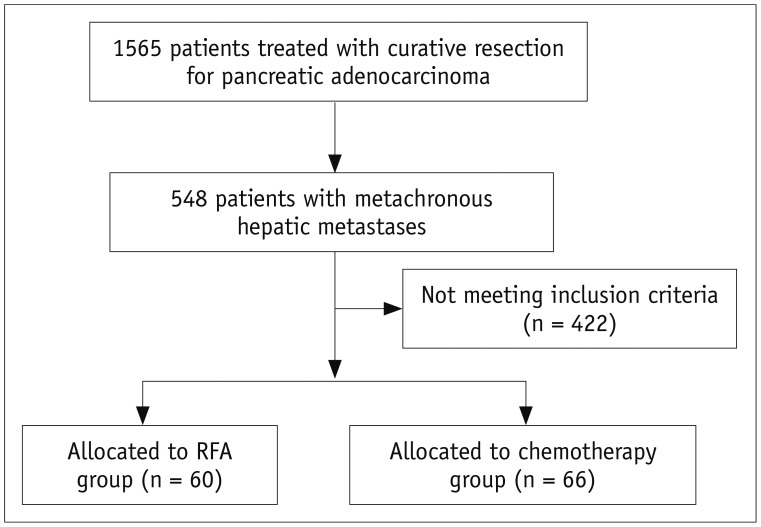
Materials and methods: Between 2002 and 2017, percutaneous RFA was performed on 94 metachronous hepatic metastases (median diameter, 1.5 cm) arising from pancreatic cancer in 60 patients (mean age, 60.5 years). Patients were included if they had fewer than five metastases, a maximum tumor diameter of ≤ 5 cm, and disease confined to the liver or stable extrahepatic disease. For comparisons during the same period, we included 66 patients who received chemotherapy only and met the same eligibility criteria described.
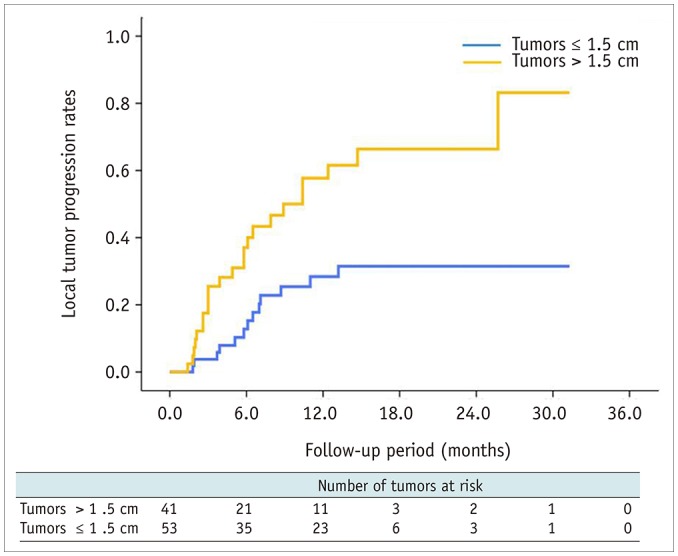
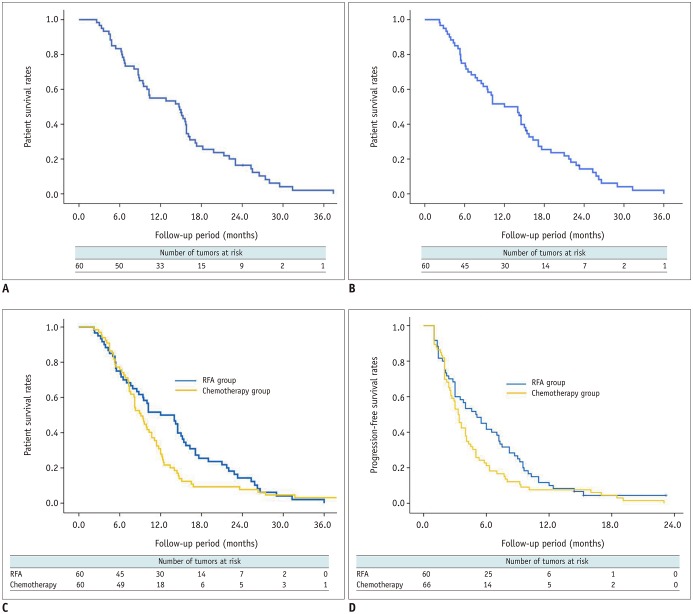
Results: Technical success was achieved in all hepatic metastasis without any procedure-related mortality. During follow-up, local tumor progression of treated lesions was observed in 38.3% of the tumors. Overall median survival and 3-year survival rates were 12 months and 0%, respectively from initial RFA, and 14.7 months and 2.1%, respectively from the first diagnosis of liver metastasis. Multivariate analysis showed that a large tumor diameter of > 1.5 cm, a late TNM stage (≥ IIB) before curative surgery, a time from surgery to recurrence of < 1 year, and the presence of extrahepatic metastasis, were all prognostic of reduced overall survival after RFA. Median overall (12 months vs. 9.1 months, p = 0.094) and progression-free survival (5 months vs. 3.3 months, p = 0.068) were higher in the RFA group than in the chemotherapy group with borderline statistical difference.
Conclusion: RFA is safe and may offer successful local tumor control in patients with metachronous hepatic metastases arising from pancreatic adenocarcinoma. Patients with a small diameter tumor, early TNM stage before curative surgery, late hepatic recurrence, and liver-only metastasis benefit most from RFA treatment. RFA provided better survival outcomes than chemotherapy for this specific group with borderline statistical difference.
Keywords: Metachronous hepatic metastasis; Pancreatic adenocarcinoma; Radiofrequency ablation.
Copyright © 2020 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Bramhall SR, Allum WH, Jones AG, Allwood A, Cummins C, Neoptolemos JP. Treatment and survival in 13,560 patients with pancreatic cancer, and incidence of the disease, in the West Midlands: an epidemiological study. Br J Surg. 1995;82:111–115. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7–30. - PubMed
-
- Lockhart AC, Rothenberg ML, Berlin JD. Treatment for pancreatic cancer: current therapy and continued progress. Gastroenterology. 2005;128:1642–1654. - PubMed
-
- Sener SF, Fremgen A, Menck HR, Winchester DP. Pancreatic cancer: a report of treatment and survival trends for 100,313 patients diagnosed from 1985-1995, using the National Cancer Database. J Am Coll Surg. 1999;189:1–7. - PubMed
-
- Sohn TA, Yeo CJ, Cameron JL, Koniaris L, Kaushal S, Abrams RA, et al. Resected adenocarcinoma of the pancreas-616 patients: results, outcomes, and prognostic indicators. J Gastrointest Surg. 2000;4:567–579. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
