

Label-Free Leukemia Monitoring by Computer Vision
- PMID: 32091180
- PMCID: PMC7213640
- DOI: 10.1002/cyto.a.23987
Label-Free Leukemia Monitoring by Computer Vision
Abstract
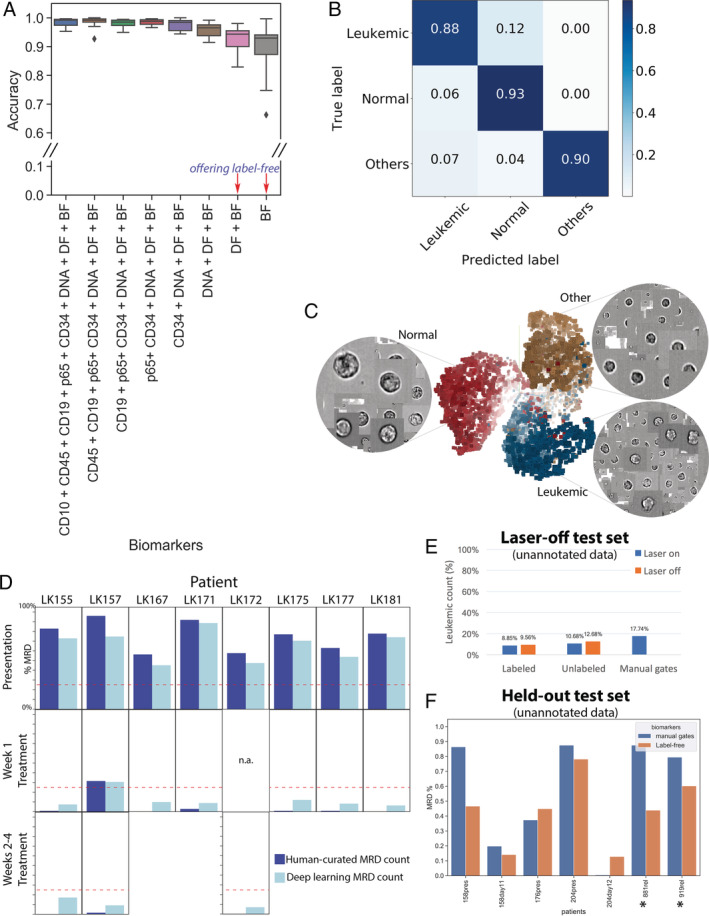
Acute lymphoblastic leukemia (ALL) is the most common childhood cancer. While there are a number of well-recognized prognostic biomarkers at diagnosis, the most powerful independent prognostic factor is the response of the leukemia to induction chemotherapy (Campana and Pui: Blood 129 (2017) 1913-1918). Given the potential for machine learning to improve precision medicine, we tested its capacity to monitor disease in children undergoing ALL treatment. Diagnostic and on-treatment bone marrow samples were labeled with an ALL-discriminating antibody combination and analyzed by imaging flow cytometry. Ignoring the fluorescent markers and using only features extracted from bright-field and dark-field cell images, a deep learning model was able to identify ALL cells at an accuracy of >88%. This antibody-free, single cell method is cheap, quick, and could be adapted to a simple, laser-free cytometer to allow automated, point-of-care testing to detect slow early responders. Adaptation to other types of leukemia is feasible, which would revolutionize residual disease monitoring. © 2020 The Authors. Cytometry Part A published by Wiley Periodicals, Inc. on behalf of International Society for Advancement of Cytometry.
Keywords: computer vision; deep learning; imaging flow cytometry; label-free; leukemia; machine learning; neural networks.
© 2020 The Authors. Cytometry Part A published by Wiley Periodicals, Inc. on behalf of International Society for Advancement of Cytometry.
Figures
References
-
- Vora A, Goulden N, Mitchell C, Hancock J, Hough R, Rowntree C, Moorman AV, Wade R. Augmented post‐remission therapy for a minimal residual disease‐defined high‐risk subgroup of children and young people with clinical standard‐risk and intermediate‐risk acute lymphoblastic leukaemia (UKALL 2003): A randomised controlled trial. Lancet Oncol 2014;15:809–818. - PubMed
-
- Vora A, Goulden N, Wade R, Mitchell C, Hancock J, Hough R, Rowntree C, Richards S. Treatment reduction for children and young adults with low‐risk acute lymphoblastic leukaemia defined by minimal residual disease (UKALL 2003): A randomised controlled trial. Lancet Oncol 2013;14:199–209. - PubMed
-
- Gupta S, Devidas M, Loh ML, Raetz EA, Chen S, Wang C, Brown P, Carroll AJ, Heerema NA, Gastier‐Foster JM, et al. Flow‐cytometric vs. ‐morphologic assessment of remission in childhood acute lymphoblastic leukemia: A report from the Children's oncology group (COG). Leukemia 2018;32:1370–1379. 10.1038/s41375-018-0039-7. - DOI - PMC - PubMed
-
- O'Connor D, Moorman AV, Wade R, Hancock J, Tan RMR, Bartram J, Moppett J, Schwab C, Patrick K, Harrison CJ, et al. Use of minimal residual disease assessment to redefine induction failure in pediatric acute lymphoblastic leukemia. J Clin Oncol 2017;35:660–667. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
