

Estimated effectiveness of symptom and risk screening to prevent the spread of COVID-19
- PMID: 32091395
- PMCID: PMC7060038
- DOI: 10.7554/eLife.55570
Estimated effectiveness of symptom and risk screening to prevent the spread of COVID-19
Abstract
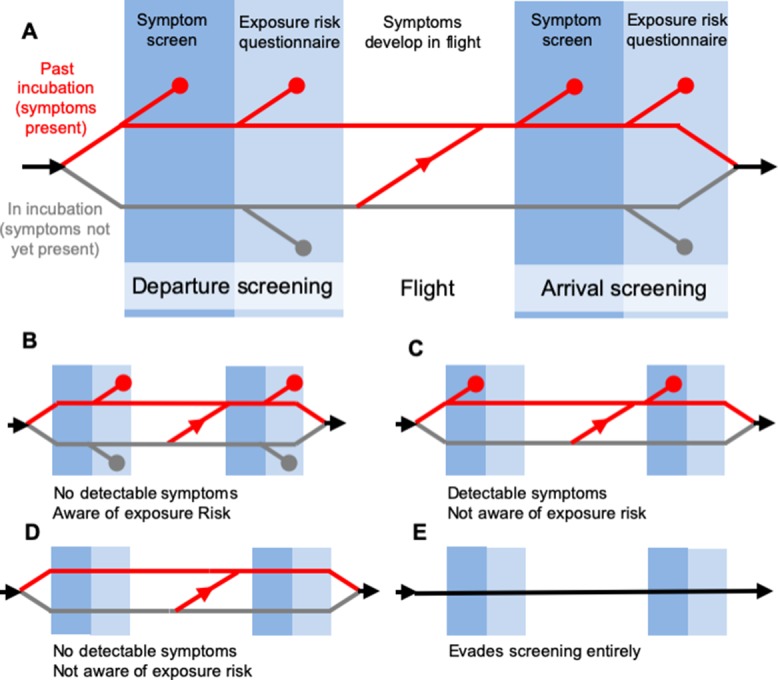
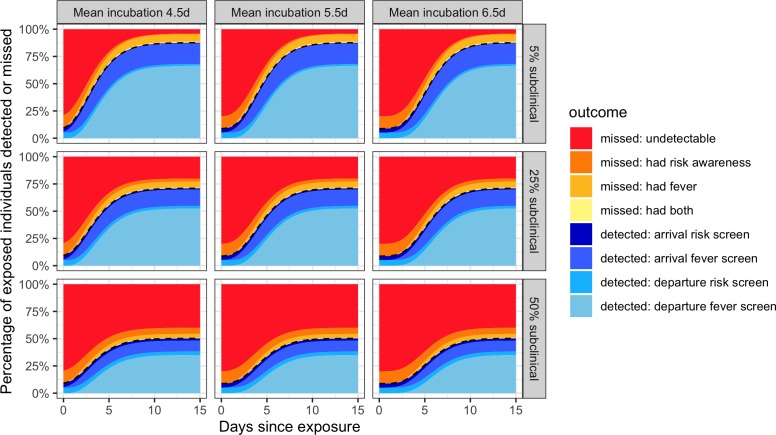
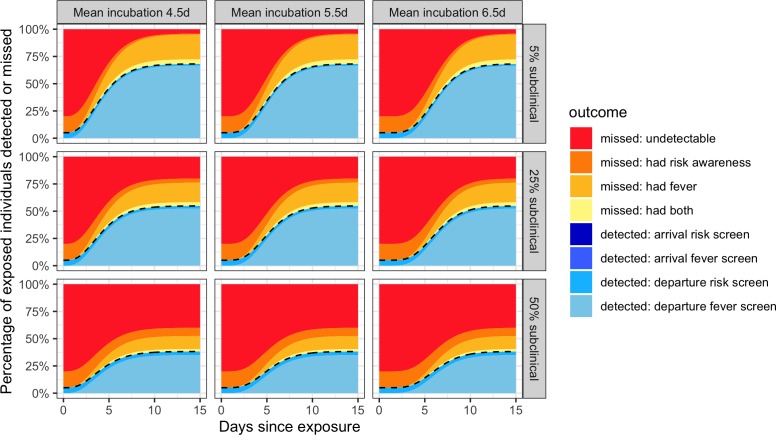
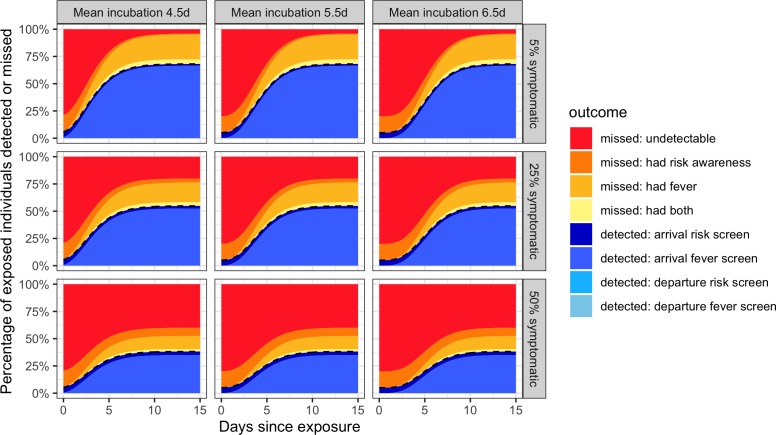
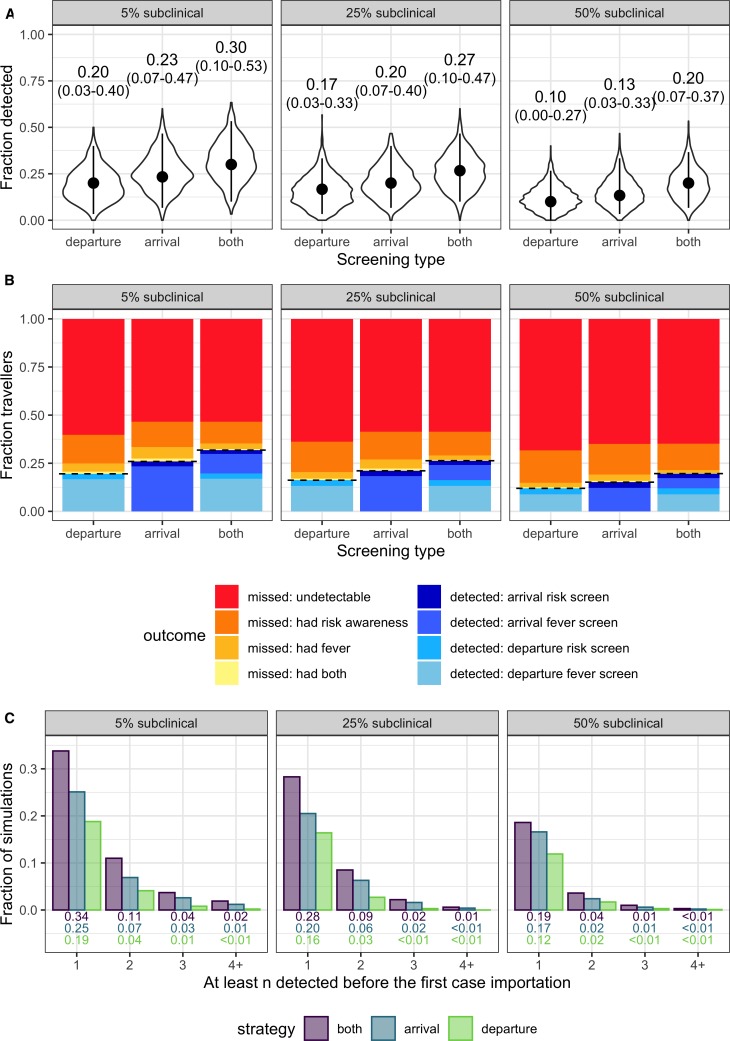
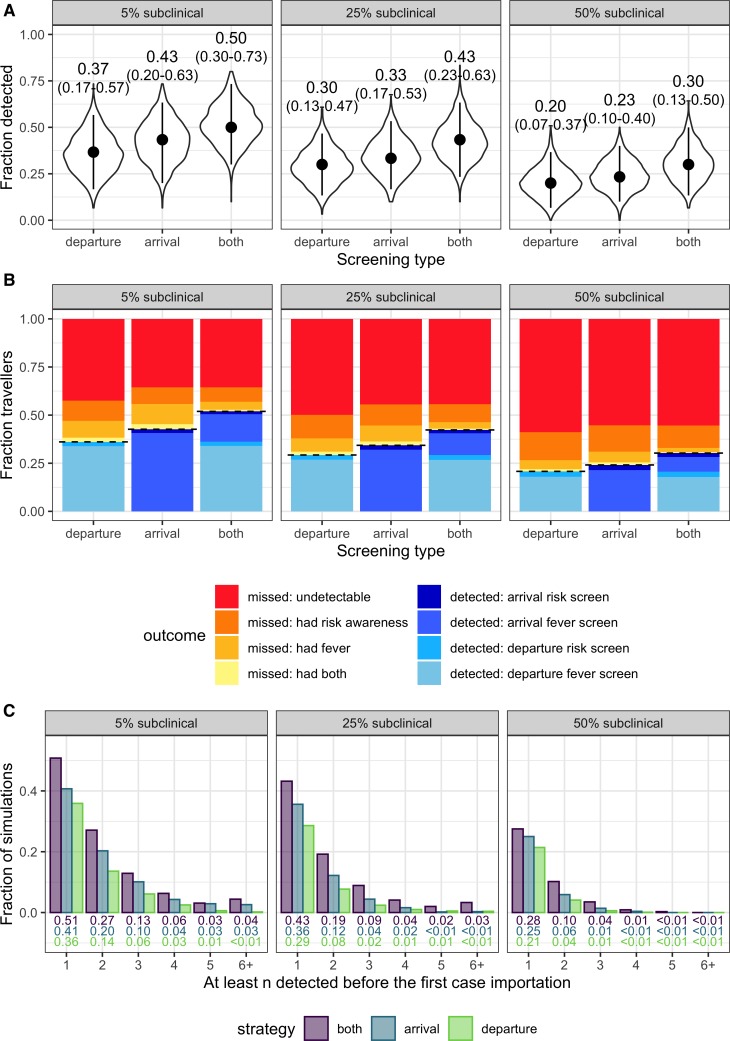
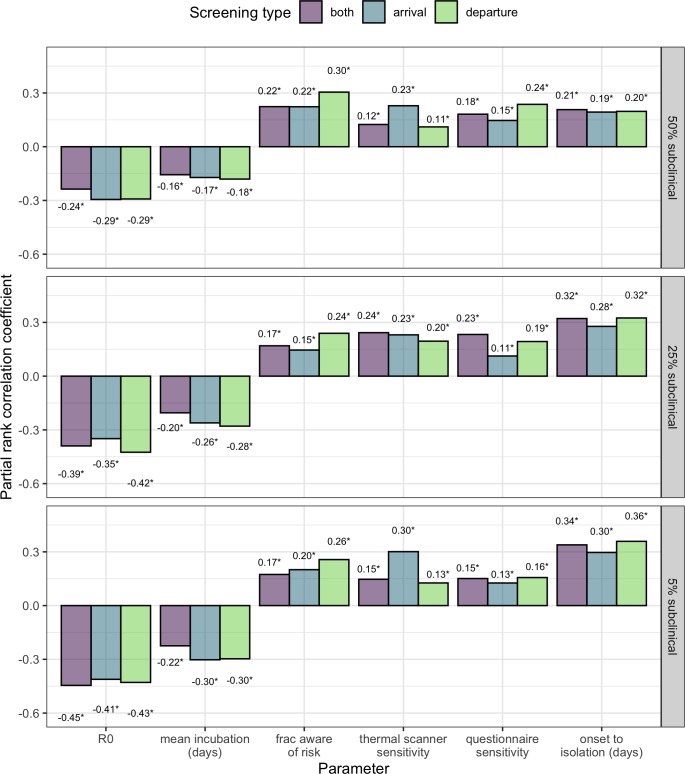
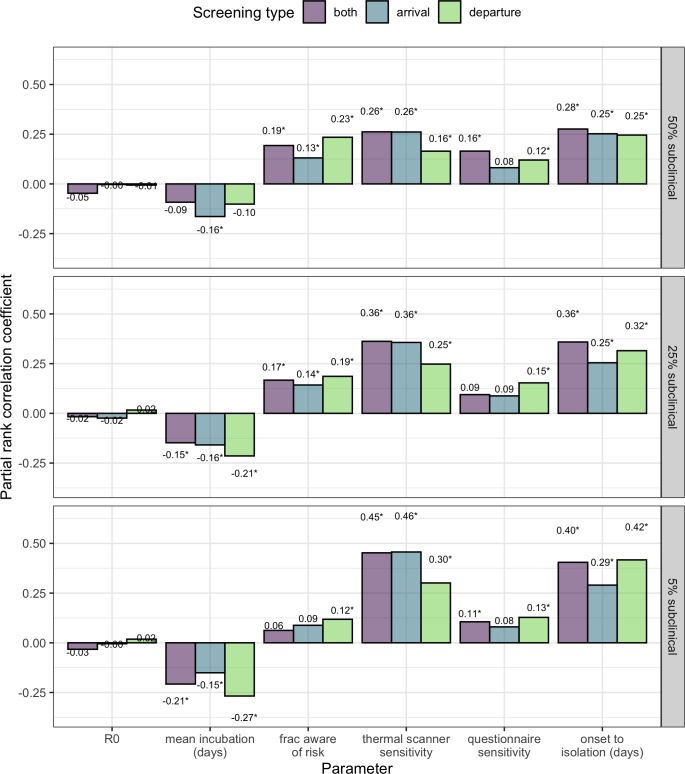
Traveller screening is being used to limit further spread of COVID-19 following its recent emergence, and symptom screening has become a ubiquitous tool in the global response. Previously, we developed a mathematical model to understand factors governing the effectiveness of traveller screening to prevent spread of emerging pathogens (Gostic et al., 2015). Here, we estimate the impact of different screening programs given current knowledge of key COVID-19 life history and epidemiological parameters. Even under best-case assumptions, we estimate that screening will miss more than half of infected people. Breaking down the factors leading to screening successes and failures, we find that most cases missed by screening are fundamentally undetectable, because they have not yet developed symptoms and are unaware they were exposed. Our work underscores the need for measures to limit transmission by individuals who become ill after being missed by a screening program. These findings can support evidence-based policy to combat the spread of COVID-19, and prospective planning to mitigate future emerging pathogens.
Keywords: COVID-19; SARS-CoV-2; emerging infectious disease; epidemic containment; epidemic control; epidemiology; global health; human; travel screening; virus.
© 2020, Gostic et al.
Conflict of interest statement
KG, AG, RM, AK, JL No competing interests declared
Figures
References
-
- BBC News China restricts movement to fight coronavirus. [February 20, 2020];2020 https://www.bbc.com/news/world-asia-china-51523835
-
- Bhatia S, Imai N, Cuomo-Dannenburg G, Baguelin M, Boonyasiri A, Cori A, Cucunubá Z, Dorigatti I, FitzJohn R, Fu H, Gaythorpe K, Ghani A, Hamlet A, Hinsley W, Laydon D, Nedjati-Gilani G, Okell L, Riley S, Thompson H, Elsland S, Volz E, Wang H, Wang Y, Whittaker C, Xi X, Donnelly C, Ferguson N. Report 6: Relativesensitivity of International Surveillance. Imperial College; 2020. https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-...
-
- Biomeme Fast detection is critical to contain deadly 2019 Wuhan coronavirus. [February 21, 2020];2020 https://blog.biomeme.com/fast-detection-is-critical-to-contain-deadly-20...
-
- Bitar D, Goubar A, Desenclos JC. International travels and fever screening during epidemics: a literature review on the effectiveness and potential use of non-contact infrared thermometers. Euro Surveillance. 2009;14:19115. - PubMed
