

The Contribution of Germline Predisposition Gene Mutations to Clinical Subtypes of Invasive Breast Cancer From a Clinical Genetic Testing Cohort
- PMID: 32091585
- PMCID: PMC7735776
- DOI: 10.1093/jnci/djaa023
The Contribution of Germline Predisposition Gene Mutations to Clinical Subtypes of Invasive Breast Cancer From a Clinical Genetic Testing Cohort
Abstract
Background: The germline cancer predisposition genes associated with increased risk of each clinical subtype of breast cancer, defined by estrogen receptor (ER), progesterone receptor (PR), and HER2, are not well defined.
Methods: A total of 54 555 invasive breast cancer patients with 56 480 breast tumors were subjected to clinical hereditary cancer multigene panel testing. Heterogeneity for predisposition genes across clinical breast cancer subtypes was assessed by comparing mutation frequencies by gene among tumor subtypes and by association studies between each tumor subtype and reference controls.
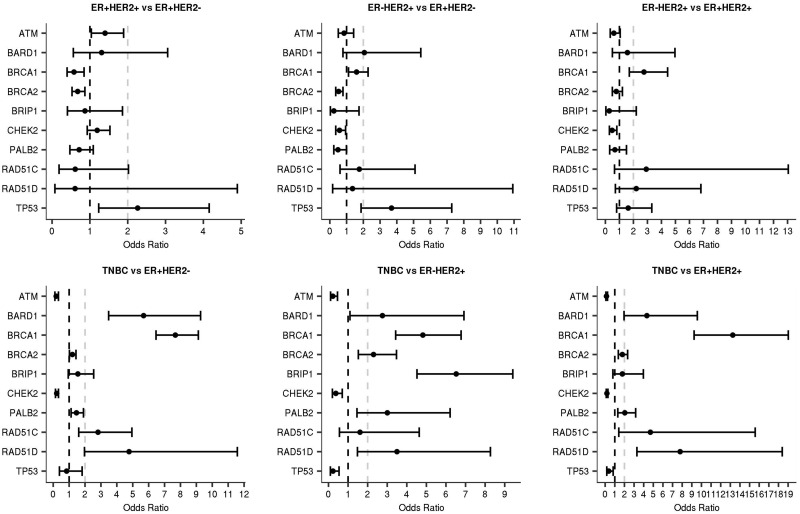
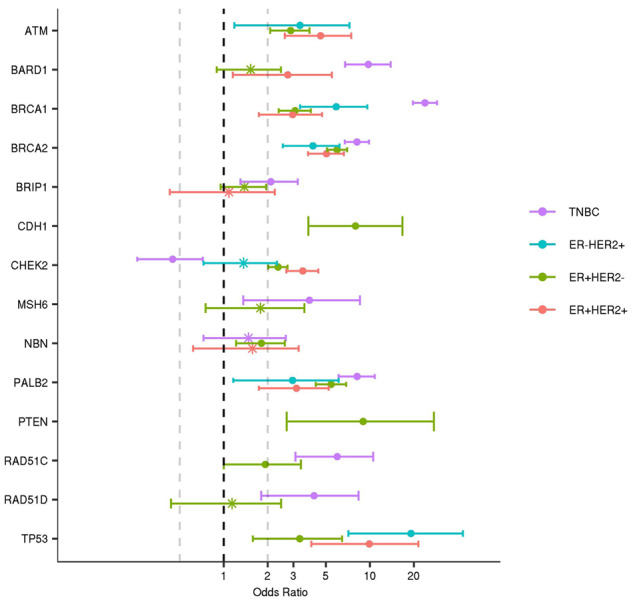
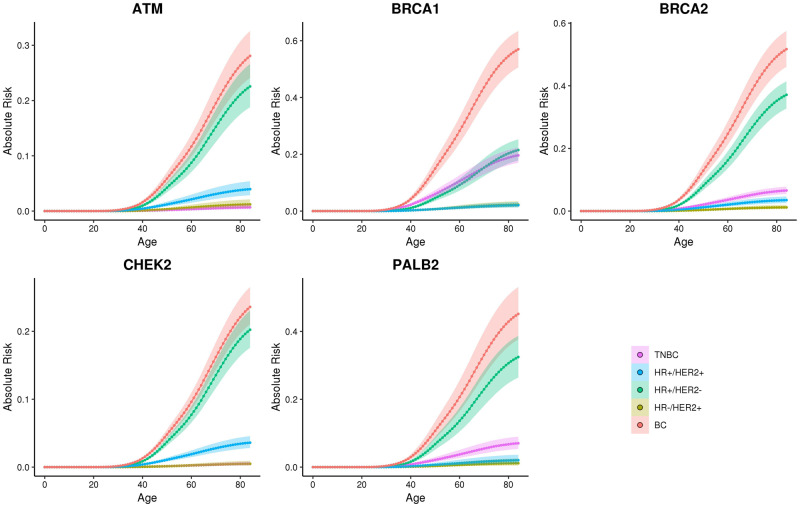
Results: Mutations in 15 cancer predisposition genes were detected in 8.6% of patients with ER+/HER2-; 8.9% with ER+/HER2+; 7.7% with ER-/HER2+; and 14.4% of ER-/PR-/HER2- tumors. BRCA1, BRCA2, BARD1, and PALB2 mutations were enriched in ER- and HER2- tumors; RAD51C and RAD51D mutations were enriched in ER- tumors only; TP53 mutations were enriched in HER2+ tumors, and ATM and CHEK2 mutations were enriched in both ER+ and/or HER2+ tumors. All genes were associated with moderate (odds ratio > 2.00) or strong (odds ratio > 5.00) risks of at least one subtype of breast cancer in case-control analyses. Mutations in ATM, BARD1, BRCA1, BRCA2, CHEK2, PALB2, RAD51C, RAD51D, and TP53 had predicted lifetime absolute risks of at least 20.0% for breast cancer.
Conclusions: Germline mutations in hereditary cancer panel genes confer subtype-specific risks of breast cancer. Combined tumor subtype, age at breast cancer diagnosis, and family history of breast and/or ovarian cancer information provides refined categorical estimates of mutation prevalence for women considering genetic testing.
© The Author(s) 2020. Published by Oxford University Press.
Figures
References
-
- Regan MM, Pagani O, Francis PA, et al. Predictive value and clinical utility of centrally assessed ER, PgR, and Ki-67 to select adjuvant endocrine therapy for premenopausal women with hormone receptor-positive, HER2-negative early breast cancer: TEXT and SOFT trials. Breast Cancer Res Treat. 2015;154(2):275–286. - PMC - PubMed
-
- Early Breast Cancer Trialists’ Collaborative G. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365(9472):1687–1717. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
