

Modulation of the antidepressant effects of ketamine by the mTORC1 inhibitor rapamycin
- PMID: 32092760
- PMCID: PMC7162891
- DOI: 10.1038/s41386-020-0644-9
Modulation of the antidepressant effects of ketamine by the mTORC1 inhibitor rapamycin
Abstract
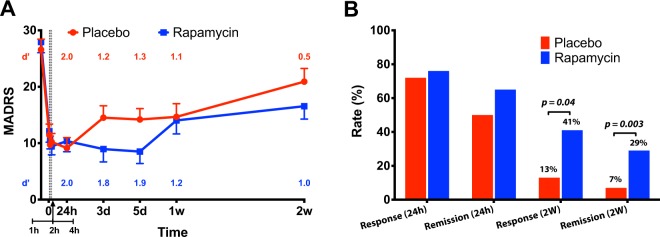
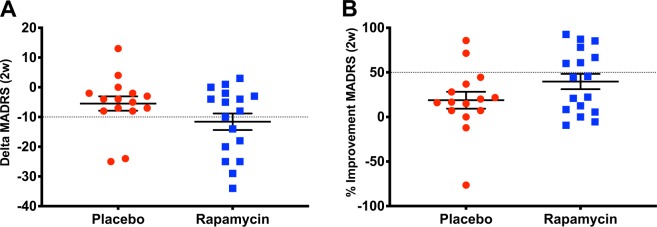
Twenty-four hours after administration, ketamine exerts rapid and robust antidepressant effects that are thought to be mediated by activation of the mechanistic target of rapamycin complex 1 (mTORC1). To test this hypothesis, depressed patients were pretreated with rapamycin, an mTORC1 inhibitor, prior to receiving ketamine. Twenty patients suffering a major depressive episode were randomized to pretreatment with oral rapamycin (6 mg) or placebo 2 h prior to the intravenous administration of ketamine 0.5 mg/kg in a double-blind cross-over design with treatment days separated by at least 2 weeks. Depression severity was assessed using Montgomery-Åsberg Depression Rating Scale (MADRS). Rapamycin pretreatment did not alter the antidepressant effects of ketamine at the 24-h timepoint. Over the subsequent 2-weeks, we found a significant treatment by time interaction (F(8,245) = 2.02, p = 0.04), suggesting a prolongation of the antidepressant effects of ketamine by rapamycin. Two weeks following ketamine administration, we found higher response (41%) and remission rates (29%) following rapamycin + ketamine compared to placebo + ketamine (13%, p = 0.04, and 7%, p = 0.003, respectively). In summary, single dose rapamycin pretreatment failed to block the antidepressant effects of ketamine, but it prolonged ketamine's antidepressant effects. This observation raises questions about the role of systemic vs. local blockade of mTORC1 in the antidepressant effects of ketamine, provides preliminary evidence that rapamycin may extend the benefits of ketamine, and thereby potentially sheds light on mechanisms that contribute to depression relapse after ketamine administration.
Figures
References
-
- Zarate CA, Jr, Singh JB, Carlson PJ, Brutsche NE, Ameli R, Luckenbaugh DA, et al. A randomized trial of an N-methyl-d-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry. 2006;63:856–64. - PubMed
-
- Romeo B, Choucha W, Fossati P, Rotge JY. Meta-analysis of short- and mid-term efficacy of ketamine in unipolar and bipolar depression. Psychiatry Res. 2015;230:682–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
