

Radioimmunotherapy of Pancreatic Ductal Adenocarcinoma: A Review of the Current Status of Literature
- PMID: 32092952
- PMCID: PMC7072553
- DOI: 10.3390/cancers12020481
Radioimmunotherapy of Pancreatic Ductal Adenocarcinoma: A Review of the Current Status of Literature
Abstract
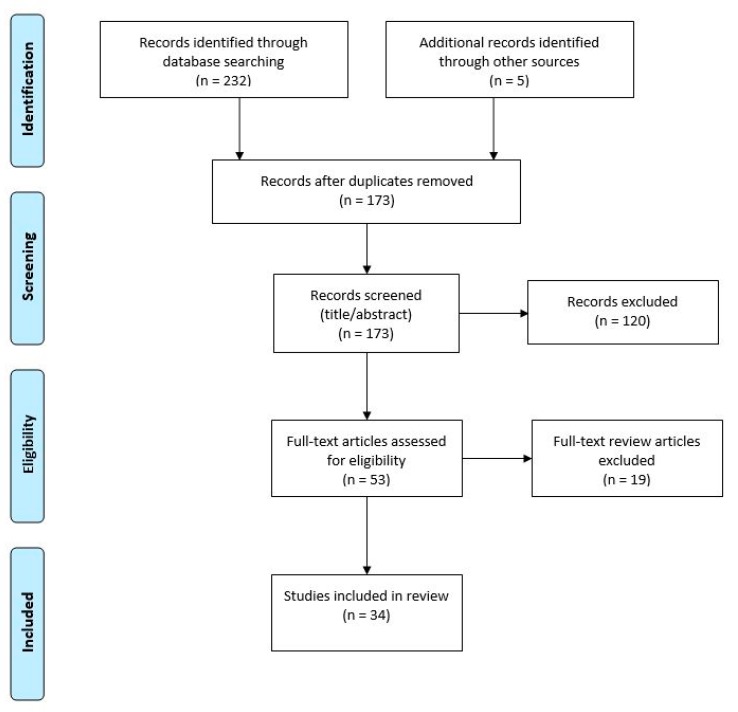
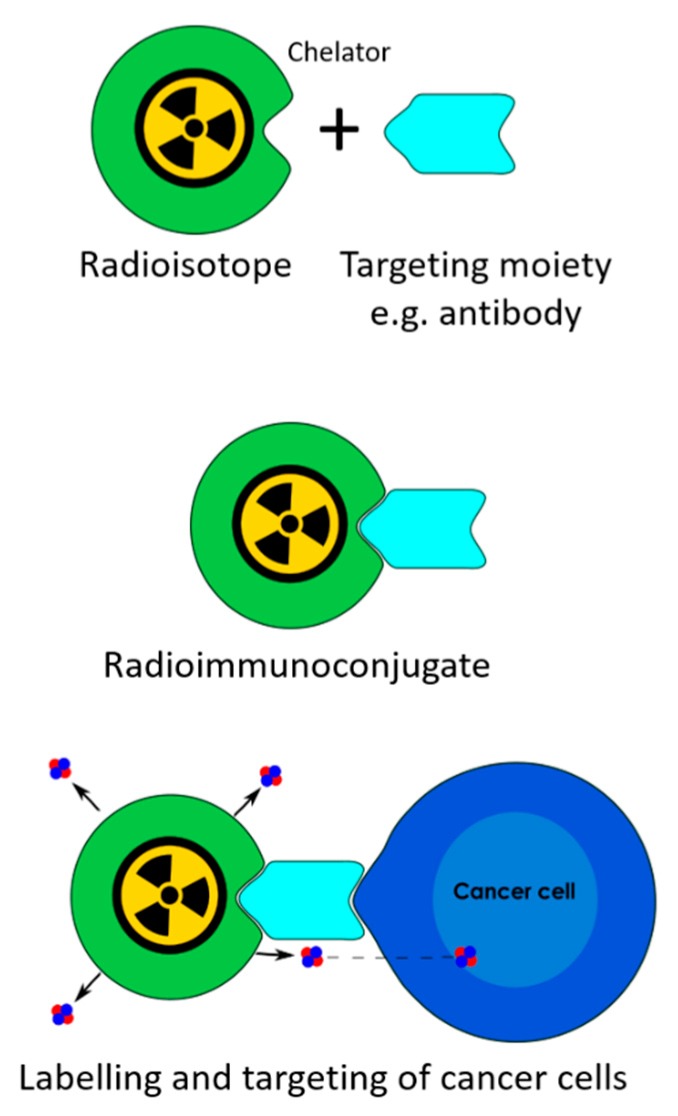
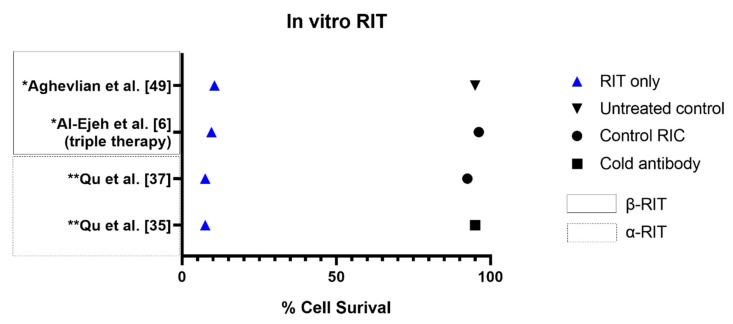
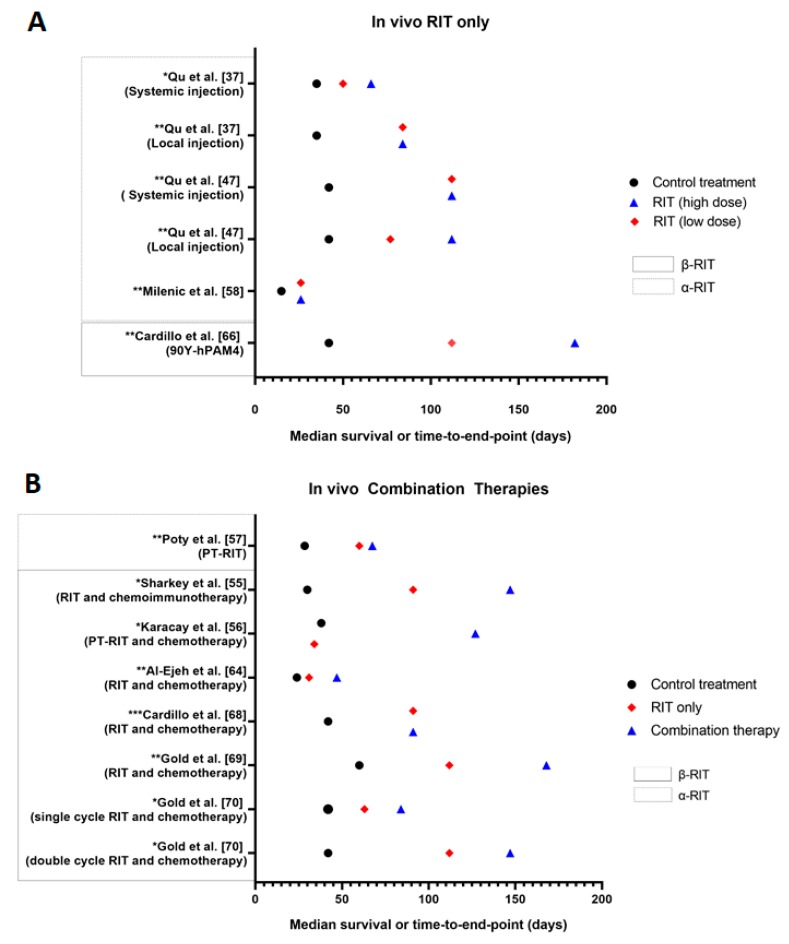
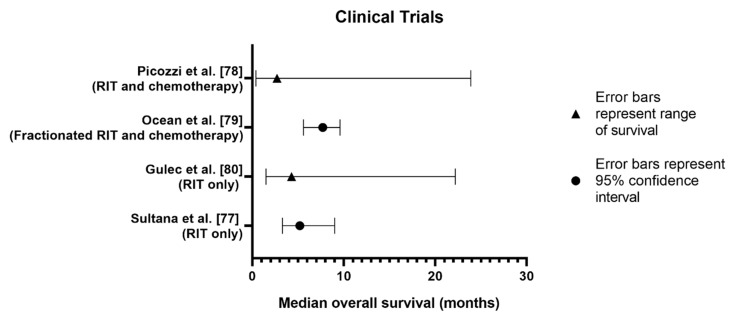
Pancreatic ductal adenocarcinoma (PDAC) has long been associated with low survival rates. A lack of accurate diagnostic tests and limited treatment options contribute to the poor prognosis of PDAC. Radioimmunotherapy using α- or β-emitting radionuclides has been identified as a potential treatment for PDAC. By harnessing the cytotoxicity of α or β particles, radioimmunotherapy may overcome the anatomic and physiological factors which traditionally make PDAC resistant to most conventional treatments. Appropriate selection of target receptors and the development of selective and cytotoxic radioimmunoconjugates are needed to achieve the desired results of radioimmunotherapy. The aim of this review is to examine the growing preclinical and clinical trial evidence regarding the application of α and β radioimmunotherapy for the treatment of PDAC. A systematic search of MEDLINE® and Scopus databases was performed to identify 34 relevant studies conducted on α or β radioimmunotherapy of PDAC. Preclinical results demonstrated α and β radioimmunotherapy provided effective tumour control. Clinical studies were limited to investigating β radioimmunotherapy only. Phase I and II trials observed disease control rates of 11.2%-57.9%, with synergistic effects noted for combination therapies. Further developments and optimisation of treatment regimens are needed to improve the clinical relevance of α and β radioimmunotherapy in PDAC.
Keywords: alpha particles; beta particles; pancreatic cancer; radioimmunotherapy; radiolabelled antibodies; targeted therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Australian Institute of Health and Welfare . Cancer in Australia: 2019. Government of Australia; Canberra, Australia: 2019.
-
- Yoshii Y., Matsumoto H., Yoshimoto M., Oe Y., Zhang M.R., Nagatsu K., Sugyo A., Tsuji A.B., Higashi T. 64Cu-intraperitoneal radioimmunotherapy: A novel approach for adjuvant treatment in a clinically relevant preclinical model of pancreatic cancer. J. Nucl. Med. 2019;60:1437–1443. doi: 10.2967/jnumed.118.225045. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
