

Relationships Among and Predictive Values of Obesity, Inflammation Markers, and Disease Severity in Pediatric Patients with Obstructive Sleep Apnea Before and After Adenotonsillectomy
- PMID: 32093397
- PMCID: PMC7073666
- DOI: 10.3390/jcm9020579
Relationships Among and Predictive Values of Obesity, Inflammation Markers, and Disease Severity in Pediatric Patients with Obstructive Sleep Apnea Before and After Adenotonsillectomy
Abstract
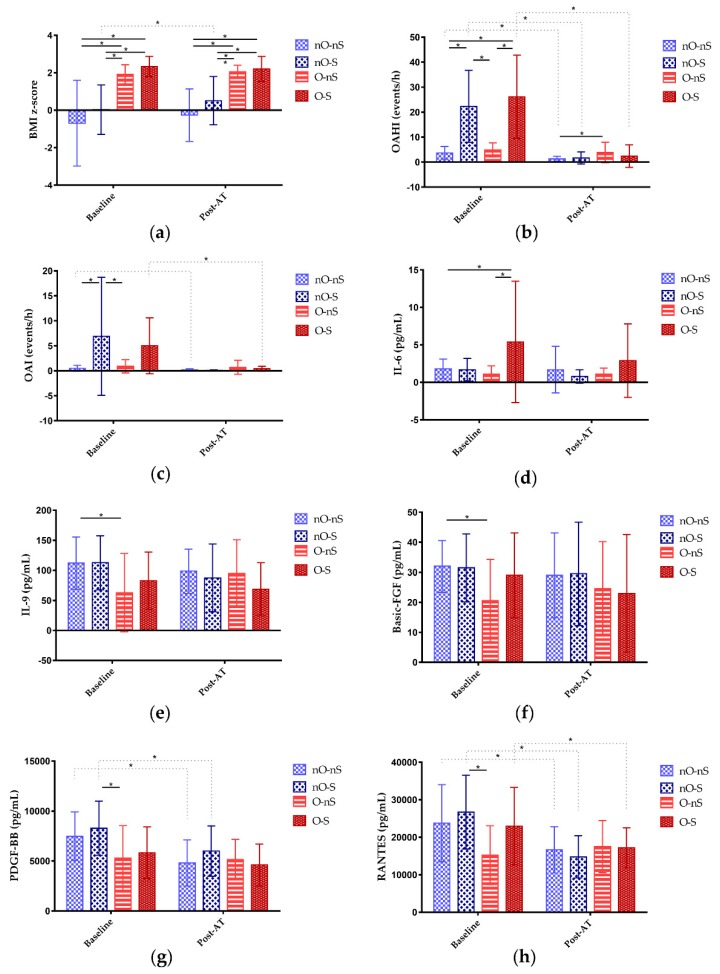
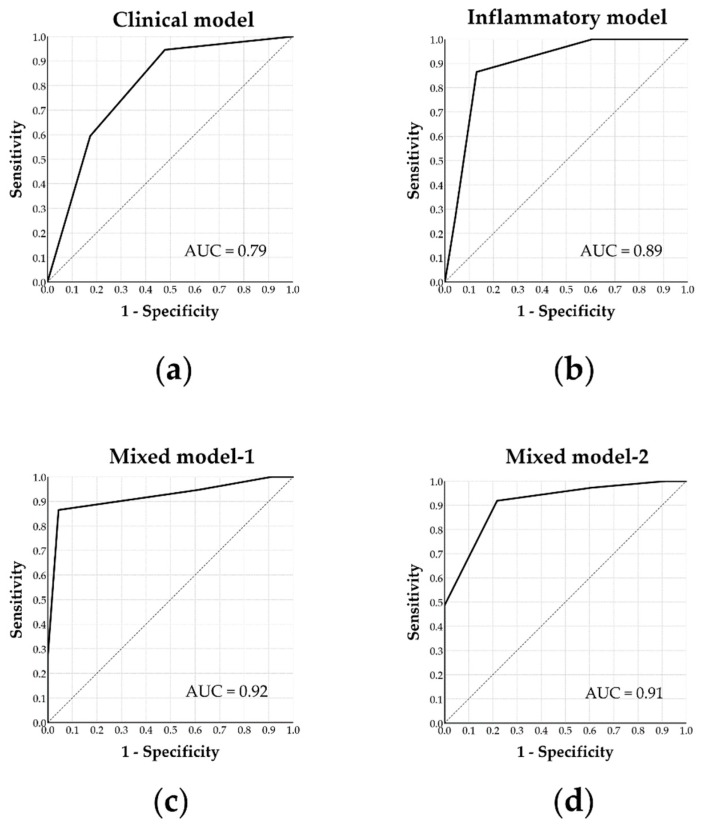
Both obstructive sleep apnea (OSA) and obesity are major health issues that contribute to increased systemic inflammation in children. To date, adenotonsillectomy (AT) is still the first-line treatment for childhood OSA. However, the relationships among and predictive values of obesity, inflammation, and OSA severity have not been comprehensively investigated. This prospective study investigated body mass index (BMI), serum inflammatory markers, and OSA severity before and after AT in 60 pediatric patients with OSA. At baseline, differences in levels of interleukin-6, interleukin-9, basic fibroblast growth factor, platelet-derived growth factor-BB, as well as regulated on activation, normal T cell expressed and secreted (RANTES) were significant among the various weight status and OSA severity subgroups. After 3 months postoperatively, the differences in these inflammatory markers diminished along with a decrease in OSA severity while obesity persisted. The rate of surgical cure (defined as postoperative obstructive apnea-hypopnea index < 2.0 and obstructive apnea index < 1.0) was 62%. Multivariate analysis revealed that age, BMI z-score, granulocyte-macrophage colony-stimulating factor, monocyte chemotactic protein-1, and RANTES independently predicted surgical cure. Despite the significant reductions in inflammatory markers and OSA severity after AT, an inter-dependent relationship between obesity and OSA persisted. In addition to age and BMI, several inflammatory markers helped to precisely predict surgical cure.
Keywords: RANTES; adenotonsillectomy; basic fibroblast growth factor; children; granulocyte-macrophage colony-stimulating factor; interleukin; monocyte chemotactic protein; obesity; obstructive sleep apnea; platelet-derived growth factor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Heinzer R., Vat S., Marques-Vidal P., Marti-Soler H., Andries D., Tobback N., Mooser V., Preisig M., Malhotra A., Waeber G., et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015;3:310–318. doi: 10.1016/S2213-2600(15)00043-0. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
