

The efficacy of continuous versus single-injection femoral nerve block in Total knee Arthroplasty: a systematic review and meta-analysis
- PMID: 32093655
- PMCID: PMC7041113
- DOI: 10.1186/s12891-020-3148-1
The efficacy of continuous versus single-injection femoral nerve block in Total knee Arthroplasty: a systematic review and meta-analysis
Abstract
Background: Continuous femoral nerve block (cFNB) has been developed to extend the analgesic effect since the efficacy of single-injection femoral nerve block (sFNB) is often limited to approximately 16-24 h. The aim of this meta-analysis was to validate the add-on effect of cFNB in the setting of a multimodal analgesic protocol.
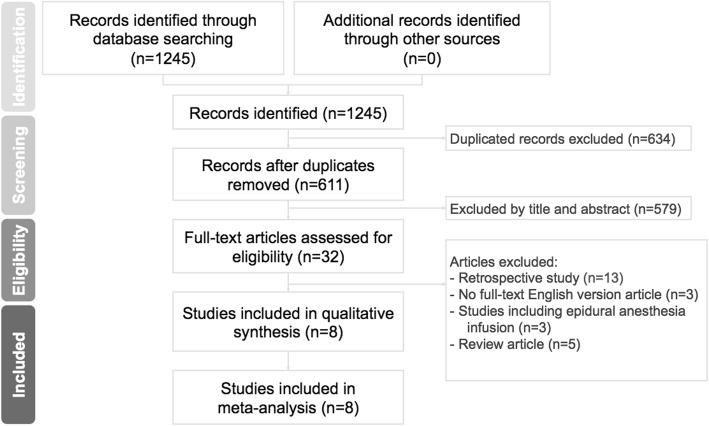
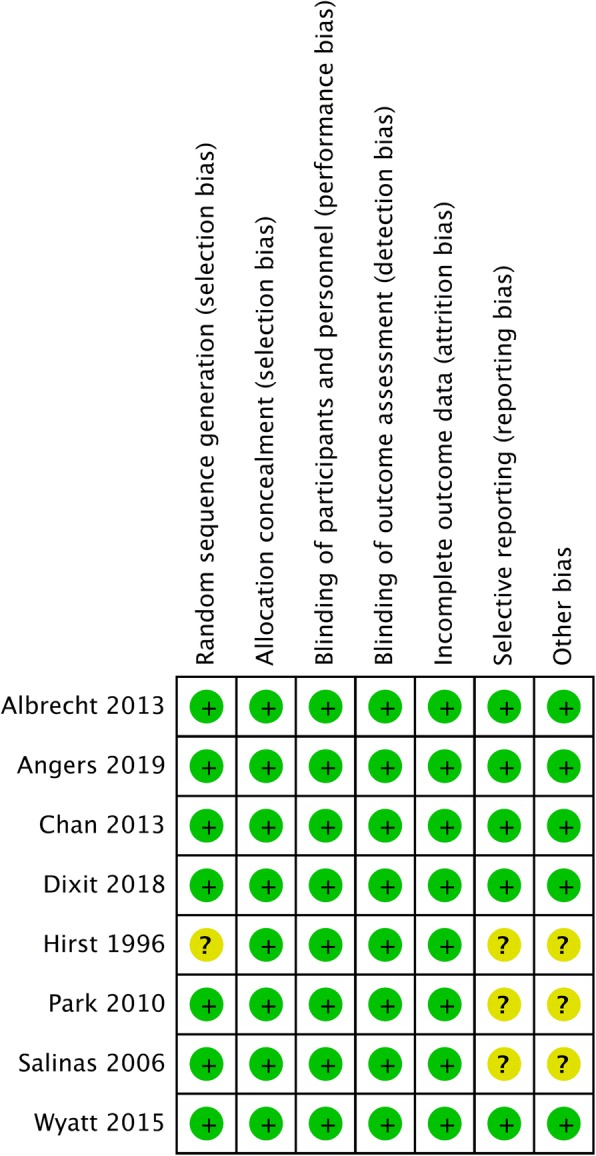
Methods: We performed a comprehensive literature review on Web of Science, Embase, the Cochrane Library and PubMed. Eight randomized controlled trials (N = 626) that compared the efficacy of cFNB with sFNB were included. The primary outcome domains consist of visual analog scale (VAS) score at postoperative 24 and 48 h. The secondary outcome domains include opioid consumption, length of hospital stay and incidence of nausea.
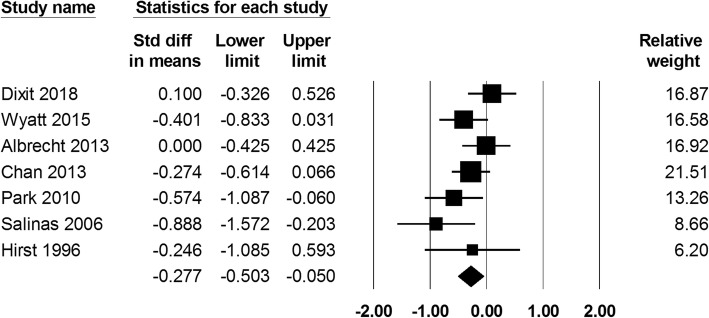
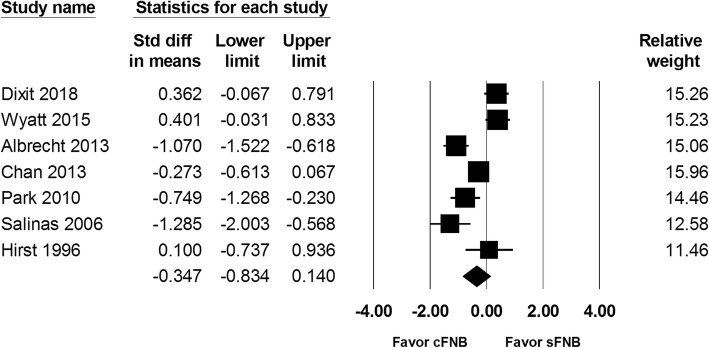
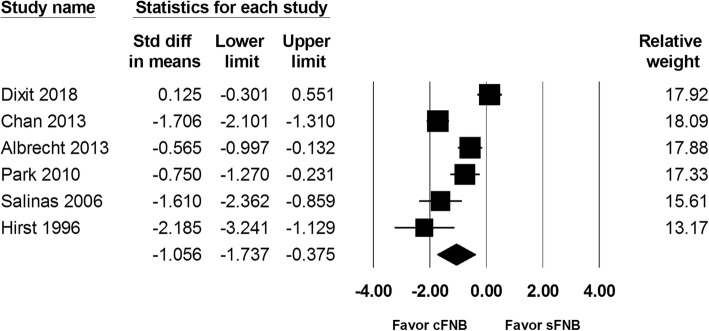
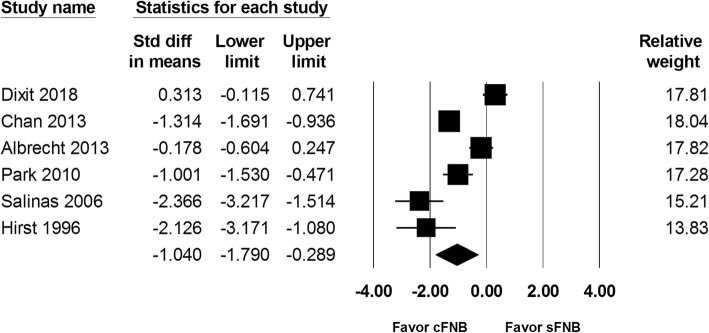
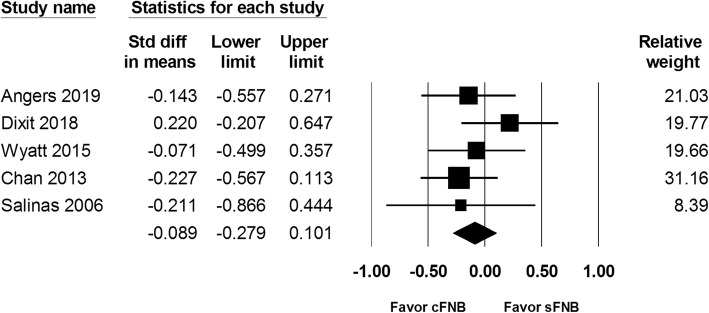
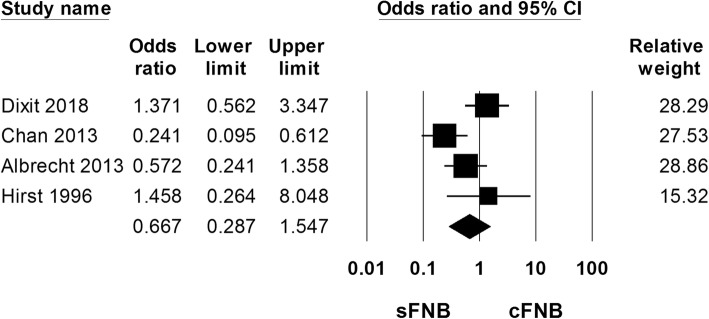
Results: Our analysis revealed that cFNB was associated with a lower VAS score at 24 h (SMD: -0.277;95% CI - 0.503 to - 0.05). However, the difference of VAS score did not meet the minimal clinically importance difference for total knee arthroplasty (TKA). VAS score at 48 h was similar between the cFNB and sFNB group. The cFNB group was associated with less amount of opioids consumed at both 24(SMD: -1.056;95% CI - 1.737 to - 0.375) and 48 h(SMD: -1.040;95% CI - 1.790 to - 0.289). Length of hospital stay and incidence of nausea were similar between the two groups.
Conclusion: In the setting of a multimodal analgesic protocol, patients might benefit from cFNB with regards to a reduced need of opioids in the early postoperative period. However, we did not find a clinically significant difference in pain scores at different time points between the cFNB and sFNB group.
Level of evidence: I; meta-analysis.
Keywords: Continuous; Femoral nerve block; Nerve block; Pain; Single-injection; Total knee arthroplasty.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Optimizing Pain and Rehabilitation After Knee Arthroplasty: A Two-Center, Randomized Trial.Anesth Analg. 2016 Nov;123(5):1316-1324. doi: 10.1213/ANE.0000000000001469. Anesth Analg. 2016. PMID: 27749351 Clinical Trial.
-
Effectiveness of continuous versus single injection femoral nerve block for total knee arthroplasty: A double blinded, randomized trial.Knee. 2018 Aug;25(4):623-630. doi: 10.1016/j.knee.2018.04.001. Epub 2018 Apr 26. Knee. 2018. PMID: 29705075 Clinical Trial.
-
The effect of single-injection femoral nerve block versus continuous femoral nerve block after total knee arthroplasty on hospital length of stay and long-term functional recovery within an established clinical pathway.Anesth Analg. 2006 Apr;102(4):1234-9. doi: 10.1213/01.ane.0000198675.20279.81. Anesth Analg. 2006. PMID: 16551930 Clinical Trial.
-
Effectiveness of continuous adductor canal block versus continuous femoral nerve block in patients with total knee arthroplasty: A PRISMA guided systematic review and meta-analysis.Medicine (Baltimore). 2019 Nov;98(48):e18056. doi: 10.1097/MD.0000000000018056. Medicine (Baltimore). 2019. PMID: 31770220 Free PMC article.
-
The role of sciatic nerve block to complement femoral nerve block in total knee arthroplasty: a meta-analysis of randomized controlled trials.J Anesth. 2018 Jun;32(3):341-350. doi: 10.1007/s00540-018-2480-1. Epub 2018 Mar 8. J Anesth. 2018. PMID: 29520522
Cited by
-
A guide to regional analgesia for Total Knee Arthroplasty.EFORT Open Rev. 2021 Dec 10;6(12):1181-1192. doi: 10.1302/2058-5241.6.210045. EFORT Open Rev. 2021. PMID: 35839095 Free PMC article.
-
Continuous Femoral Nerve Block Reduces the Need for Manipulation Following Total Knee Arthroplasty.JB JS Open Access. 2022 Aug 4;7(3):e21.00155. doi: 10.2106/JBJS.OA.21.00155. eCollection 2022 Jul-Sep. JB JS Open Access. 2022. PMID: 35935602 Free PMC article.
-
Continuous femoral nerve block as pain management following total knee arthroplasty: a systematic review.Arch Orthop Trauma Surg. 2025 Apr 11;145(1):238. doi: 10.1007/s00402-025-05855-3. Arch Orthop Trauma Surg. 2025. PMID: 40214694
-
Sublingual Sufentanil Tablet System (SSTS-Zalviso®) for Postoperative Analgesia after Orthopedic Surgery: A Retrospective Study.J Clin Med. 2022 Nov 21;11(22):6864. doi: 10.3390/jcm11226864. J Clin Med. 2022. PMID: 36431339 Free PMC article.
-
Effects of dexmedetomidine as a perineural adjuvant for femoral nerve block: A systematic review and meta-analysis.PLoS One. 2020 Oct 19;15(10):e0240561. doi: 10.1371/journal.pone.0240561. eCollection 2020. PLoS One. 2020. PMID: 33075089 Free PMC article.
References
-
- American Society of Anesthesiologists Task Force on Acute Pain M Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on acute pain management. Anesthesiology. 2012;116(2):248–273. doi: 10.1097/ALN.0b013e31823c1030. - DOI - PubMed
-
- Strassels SA, Chen C, Carr DB. Postoperative analgesia: economics, resource use, and patient satisfaction in an urban teaching hospital. Anesth Analg. 2002;94(1):130–137. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
