

Effect of community active case-finding strategies for detection of tuberculosis in Cambodia: study protocol for a pragmatic cluster randomized controlled trial
- PMID: 32093778
- PMCID: PMC7041270
- DOI: 10.1186/s13063-020-4138-1
Effect of community active case-finding strategies for detection of tuberculosis in Cambodia: study protocol for a pragmatic cluster randomized controlled trial
Abstract
Background: Cambodia has made notable progress in the fight against tuberculosis (TB). However, these gains are impeded by a significant proportion of undiagnosed cases. To effectively reach people with TB, active case-finding (ACF) strategies have been adopted by countries affected by the epidemic, including Cambodia, alongside passive case finding (PCF). Despite increased efforts to improve case detection, approximately 40% of TB cases in Cambodia remained undiagnosed in 2018. In Cambodia, several community-based TB ACF modalities have been implemented, but their effectiveness has yet to be systematically assessed.
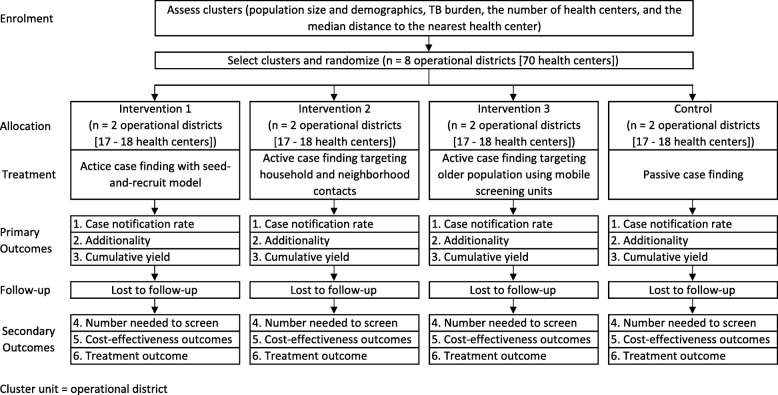
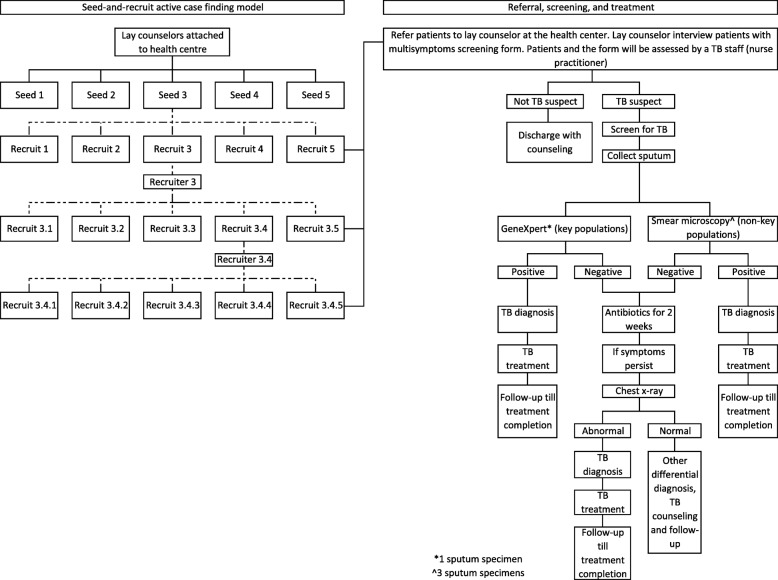
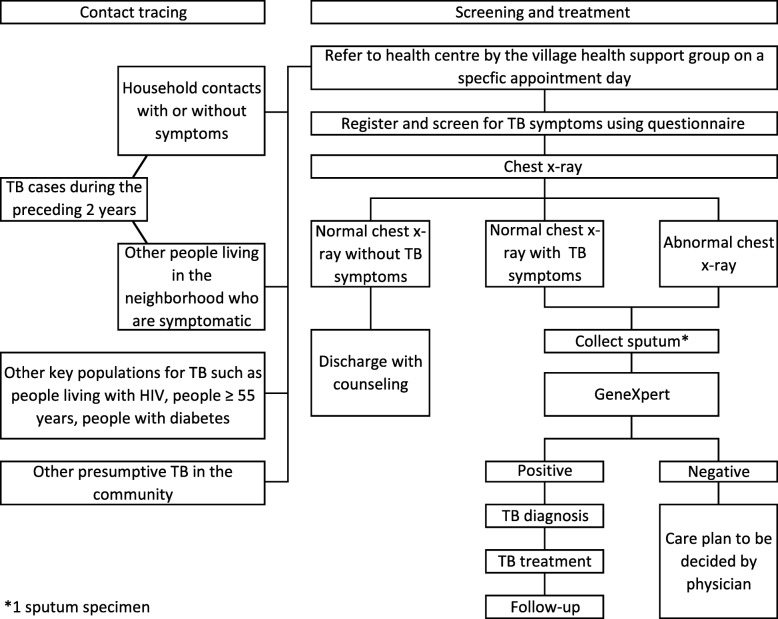
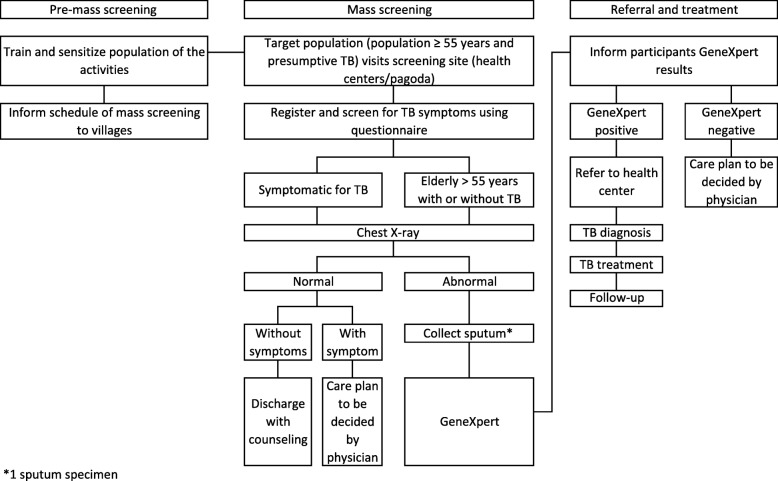
Methods: This pragmatic cluster randomized controlled trial will be conducted between December 2019 and June 2021. We will randomize eight operational districts (clusters) in seven provinces (Kampong Cham, Kampong Thom, Prey Veng, Thbong Khmum, Kampong Chhnang, Kandal, and Kampong Speu) to either the control group (PCF) or the intervention groups (ACF using a seed-and-recruit model, ACF targeting household and neighborhood contacts, and ACF targeting persons aged ≥ 55 years using mobile screening units). The primary endpoints will be TB case notification rates, additionality, and cumulative yield of TB cases. The secondary endpoints include treatment outcomes, the number needed to screen to find one TB case, and cost-effectiveness outcome measures. We will analyze the primary and secondary endpoints by intention to treat. We will compare cluster and individual-level characteristics using Student's t test and hierarchical or mixed-effect models to estimate the ratio of these means. The incremental cost-effectiveness ratio per disability-adjusted life year averted will also be considered as a benchmark to determine whether the interventions are cost-effective.
Discussion: This study will build an evidence base to inform future scale-up, implementation, and sustainability of ACF strategies in Cambodia and other similar settings. Implementation of this study will also complement TB control strategies in Cambodia by conducting ACF in operational districts without active interventions to find TB cases currently. Those who are ill and might have TB will be promptly screened, diagnosed, and linked to care. Early diagnosis and treatment initiation will also benefit their community by interrupting transmission and prevent further infections. The experience gained from this project will inform future attempts in conducting pragmatic trials in low-resource settings.
Trial registration: ClinicalTrials.gov, NCT04094350. Registered on 18 September 2019.
Keywords: Active case finding; Community; Passive case finding; Systematic screening; Tuberculosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization. Global tuberculosis report 2018. Geneva: World Health Organization; 2019.
-
- World Health Organization. TB country profile: Cambodia. Geneva: World Health Organization; 2019.
-
- Stop TB Partnership, United Nations Office for Project Services (UNOPS) 90–90–90. The tuberculosis report for heads of state and governments. Geneva: Stop TB Partnership and UNOPS; 2017.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
