

Toward operationalizing deficient emotional self-regulation in newly referred adults with ADHD: A receiver operator characteristic curve analysis
- PMID: 32093797
- PMCID: PMC7315889
- DOI: 10.1192/j.eurpsy.2019.11
Toward operationalizing deficient emotional self-regulation in newly referred adults with ADHD: A receiver operator characteristic curve analysis
Abstract
Background: A growing body of research suggests that deficient emotional self-regulation (DESR) is common and morbid among attention-deficit/hyperactivity disorder (ADHD) patients. The main aim of the present study was to assess whether high and low levels of DESR in adult ADHD patients can be operationalized and whether they are clinically useful.
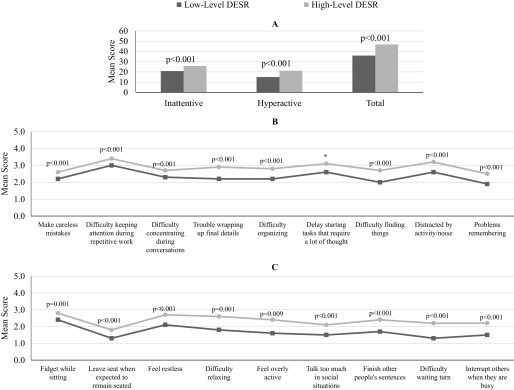
Methods: A total of 441 newly referred 18- to 55-year-old adults of both sexes with Diagnostic and Statistical Manual of Mental Disorders: Fifth Edition (DSM-5) ADHD completed self-reported rating scales. We operationalized DESR using items from the Barkley Current Behavior Scale. We used receiver operator characteristic (ROC) curves to identify the optimal cut-off on the Barkley Emotional Dysregulation (ED) Scale to categorize patients as having high- versus low-level DESR and compared demographic and clinical characteristics between the groups.
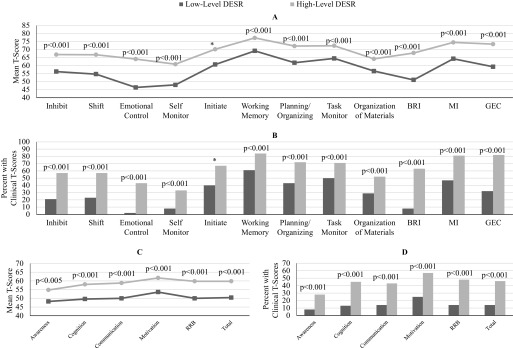
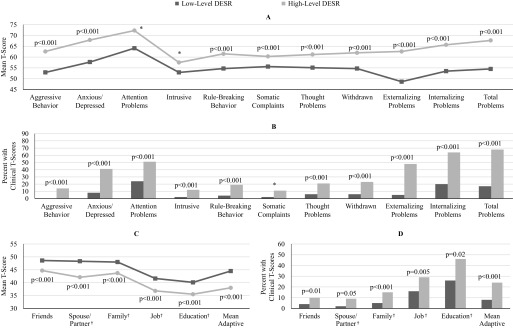
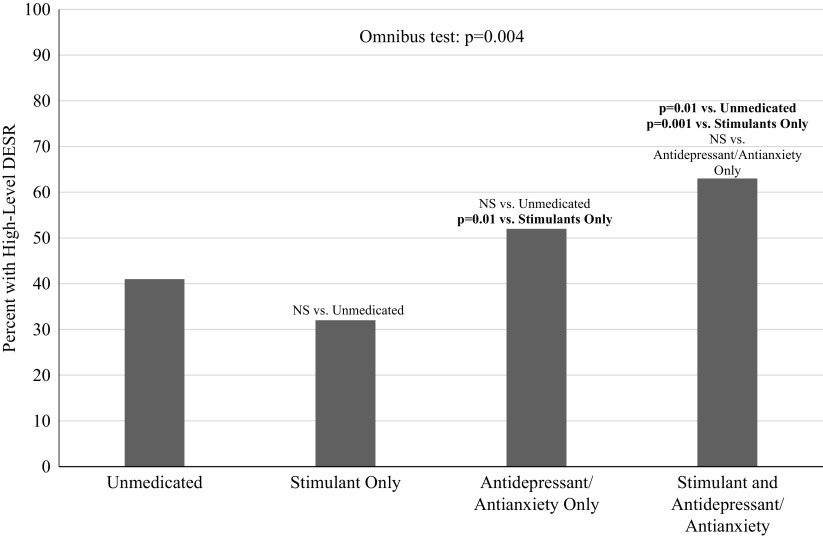
Results: We averaged the optimal Barkley ED Scale cut-points from the ROC curve analyses across all subscales and categorized ADHD patients as having high- (N = 191) or low-level (N = 250) DESR (total Barkley ED Scale score ≥8 or <8, respectively). Those with high-level DESR had significantly more severe symptoms of ADHD, executive dysfunction, autistic traits, levels of psychopathology, and worse quality of life compared with those with low-level DESR. There were no major differences in outcomes among medicated and unmedicated patients.
Conclusions: High levels of DESR are common in adults with ADHD and when present represent a burdensome source of added morbidity and disability worthy of further clinical and scientific attention.
Keywords: ADHD; comorbidity; psychopharmacology.
Conflict of interest statement
Dr. Joseph Biederman is currently receiving research support from the following sources: AACAP, Feinstein Institute for Medical Research, Food & Drug Administration, Genentech, Headspace Inc., Lundbeck AS, Neurocentria Inc., NIDA, Pfizer Pharmaceuticals, Roche TCRC Inc., Shire Pharmaceuticals Inc., Sunovion Pharmaceuticals Inc., and NIH. Dr. Biederman has a financial interest in Avekshan LLC, a company that develops treatments for attention deficit hyperactivity disorder (ADHD); his interests were reviewed and are managed by Massachusetts General Hospital and Partners HealthCare in accordance with their conflict of interest policies. Dr. Biederman’s program has received departmental royalties from a copyrighted rating scale used for ADHD diagnoses, paid by Bracket Global, Ingenix, Prophase, Shire, Sunovion, and Theravance; these royalties were paid to the Department of Psychiatry at MGH. In 2019, Dr. Biederman is a consultant for Akili, Jazz Pharma, and Shire. Through MGH corporate licensing, he has a US Patent (#14/027676) for a nonstimulant treatment for ADHD, and a patent pending (#61/233686) on a method to prevent stimulant abuse. In 2018, Dr. Biederman was a consultant for Akili and Shire. In 2017, Dr. Biederman received research support from the Department of Defense and PamLab. He was a consultant for Aevi Genomics, Akili, Guidepoint, Ironshore, Medgenics, and Piper Jaffray. He was on the scientific advisory board for Alcobra and Shire. He received honoraria from the MGH Psychiatry Academy for tuition-funded CME courses. In 2016, Dr. Biederman received honoraria from the MGH Psychiatry Academy for tuition-funded CME courses, and from Alcobra and APSARD. He was on the scientific advisory board for Arbor Pharmaceuticals. He was a consultant for Akili and Medgenics. He received research support from Merck and SPRITES.
In the past year, Dr. Faraone received income, potential income, travel expenses continuing education support, and/or research support from Tris, Otsuka, Arbor, Ironshore, Shire, Akili Interactive Labs, Enzymotec, Sunovion, Supernus, and Genomind. With his institution, he has US Patent US20130217707 A1 for the use of sodium-hydrogen exchange inhibitors in the treatment of ADHD. He also receives royalties from books published by Guilford Press: “Straight Talk about Your Child’s Mental Health,” Oxford University Press: “Schizophrenia: The Facts,” and Elsevier: “ADHD: Nonpharmacologic Interventions.” He is principal investigator of
Dr. Thomas Spencer has, in the last 3 years, received research support or was a consultant from the following sources: Avekshan, Ironshore, Lundbeck, Shire Laboratories Inc., Sunovion, the FDA, and the Department of Defense. Consultant fees are paid to the MGH Clinical Trials Network and not directly to Dr. Spencer. Dr. Spencer received support from Royalties and Licensing fees on copyrighted ADHD scales through MGH Corporate Sponsored Research and Licensing. Through MGH corporate licensing, Dr. Spencer has a US Patent (#14/027676) for a nonstimulant treatment for ADHD and a patent pending (#61/233686) for a method to prevent stimulant abuse.
Dr. Ronna Fried is currently receiving research support from Shire Pharmaceuticals and Roche Pharmaceuticals. In the past, Dr. Fried has received grant support from the Food & Drug Administration, Lundbeck AS, and the National Institutes of Health. Previously, she had been on the scientific advisory board for Johnson & Johnson and Lundbeck AS. She also had received honoraria from the MGH Psychiatry Academy for tuition-funded CME courses.
Dr. Craig Surman has received, in his lifetime, consulting fees or honorarium from McNeil, Nutricia, Pfizer, Rhodes, Shire, Somaxon, Takeda, Sunovion, and NLS. He has also received payments for lectures for Alcobra, McNeil, Janssen, Janssen-Ortho, Novartis, Shire, GME Psychiatry, and Reed/MGH Academy (funded by multiple companies). Royalties have been given to Dr. Surman from Berkeley/Penguin for “Fastminds” How to Thrive if You have ADHD (or think you might)” and from Humana/Springer for “ADHD in Adults: A Practical Guide to Evaluation and Management.” Additionally, Dr. Surman has conducted clinical research at Massachusetts General Hospital supported by Abbot, Cephalon, Hilda and Preston Davis Foundation, Eli Lilly, Magceutics, Johnson & Johnson/McNeil, Lundbeck, Merck, and Nordic Naturals.
Dr. Mai Uchida, Ms. Maura DiSalvo, Ms. K. Yvonne Woodworth, and Mr. Itai Biederman have no potential conflicts of interest to report.
Figures

References
-
- Barkley RA. Attention deficit-hyperactivity disorder: a handbook for diagnosis and treatment. 3rd ed. New York, NY: Guilford Press; 2006.
-
- Faraone SV, Rostain AL, Blader J, Busch B, Childress AC, Connor DF, et al. Practitioner review: emotional dysregulation in attention-deficit/hyperactivity disorder—implications for clinical recognition and intervention. J Child Psychol Psychiatry. 2019;60(2):133–150. - PubMed
-
- Wender PH. Attention-deficit hyperactivity disorder in adults. New York, NY: Oxford University Press; 1995.
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders: fourth edition text revision (DSM-IV-TR). 4th ed. Washington, DC: American Psychiatric Association; 2000; p. 1–943.
-
- Barkley RA. Emotional dysregulation is a core component of ADHD In: Barkley RA, editor. Attention-deficit hyperactivity disorder: a handbook for diagnosis and treatment. 4th ed. New York, NY: Guilford Press; 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
