

BRASH syndrome
- PMID: 32094236
- PMCID: PMC7046371
- DOI: 10.1136/bcr-2019-233825
BRASH syndrome
Abstract
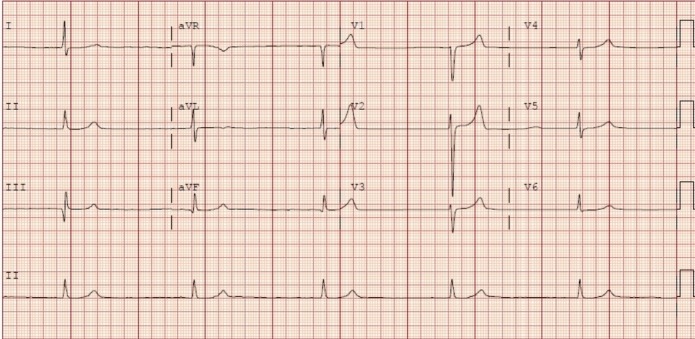
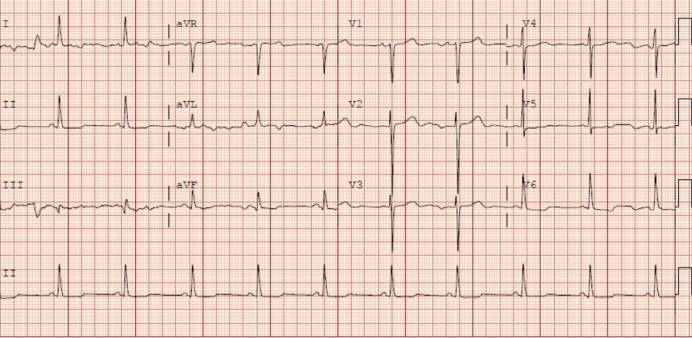
A 62-year-old woman with chronic kidney disease stage 4, sleep apnoea on continuous positive airway pressure and recent admission for acute-on-chronic diastolic heart failure presented to emergency room with weakness. She was hypotensive and had symptomatic bradycardia in the 30 s secondary to hyperkalaemia and beta-blockers, raising concern for BRASH syndrome. Antihypertensives were immediately held. Potassium-lowering agents (with calcium gluconate for cardiac stability) were begun, as were fluids and dopamine for vasopressor support. The patient was admitted to intensive care unit and electrophysiology was consulted. Over the next 2 days, the patient clinically improved: she remained off dopamine for over 24 hours; potassium levels and renal function improved; and heart rate stabilised in 60 s. The patient was eventually discharged and advised to avoid metolazone, bumetanide and carvedilol, with primary care provider and cardiology follow-up.
Keywords: adult intensive care; fluid electrolyte and acid-base disturbances; pacing and electrophysiology.
© BMJ Publishing Group Limited 2020. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Golchin A, Zhou M, Khan A. Bradycardia, Renal Failure, AV-Nodal Blockers, Shock, and Hyperkalemia (BRASH) - A New Clinical Syndrome. ATS Journals 2018;B47.
-
- Link MS, Berkow LC, Kudenchuk PJ, et al. Adult advanced cardiovascular life support. CPR and first aid, emergency cardiovascular care, 2015. Available: https://eccguidelines.heart.org/circulation/cpr-ecc-guidelines/part-7-ad... [Accessed 31 Jan 2020].
-
- Farkas J. PulmCrit- BRASH syndrome: bradycardia, renal failure, AV blocker, shock, hyperkalemia. Available: https://emcrit.org/pulmcrit/brash-syndrome-bradycardia-renal-failure-av-... [Accessed 27 Nov 2019].
-
- Gonuguntla K, Patil S, Manek G, et al. BRASH syndrome: lost in plain sight. Chest 2019;156:A2228 10.1016/j.chest.2019.08.2152 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical