

Cryptogenic stroke and atrial fibrillation in a real-world population: the role of insertable cardiac monitors
- PMID: 32094376
- PMCID: PMC7040015
- DOI: 10.1038/s41598-020-60180-6
Cryptogenic stroke and atrial fibrillation in a real-world population: the role of insertable cardiac monitors
Abstract
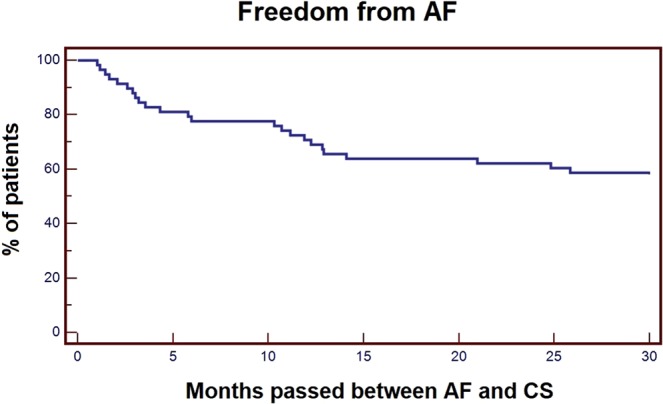
The incidence of atrial fibrillation (AF) in cryptogenic stroke (CS) patients has been studied in carefully controlled clinical trials, but real-world data are limited. We investigated the incidence of AF in clinical practice among CS patients with an insertable cardiac monitor (ICM) placed for AF detection. Patients with CS admitted to our Stroke Unit were included in the study; they received an ICM and were monitored for up to 3 years for AF detection. All detected AF episodes of at least 120 sec were considered. From March 2016 to March 2019, 58 patients (mean age 68.1 ± 9.3 years, 67% male) received an ICM to detect AF after a CS. No patients were lost to follow-up. AF was detected in 24 patients (41%, AF group mean age 70.8 ± 9.4 years, 62% male) after a mean time of 6 months from ICM (ranging from 2 days to 2 years) and 8 months after CS (ranging from 1 month to 2 years). In these AF patients, anticoagulant treatment was prescribed and nobody had a further stroke. In conclusion, AF episodes were detected via continuous monitoring with ICMs in 41% of implanted CS patients. AF in CS patients is asymptomatic and difficult to diagnose by strategies based on intermittent short-term recordings. Therefore, we suggest that ICMs should be part of daily practice in the evaluation of CS patients.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
