

Robotic Surgery: A Novel Approach for Breast Surgery and Reconstruction
- PMID: 32095394
- PMCID: PMC7015621
- DOI: 10.1097/GOX.0000000000002578
Robotic Surgery: A Novel Approach for Breast Surgery and Reconstruction
Abstract
Breast cancer is the most prevalent cancer and second leading cause of cancer-related deaths in both the US and UK female population, a prominent cause of morbidity and cost to both health services. All surgically fit patients are offered breast reconstruction following the initial surgery, and this is traditionally an open approach: either implant-based or an autologous tissue flap. Both lead to scarring that is difficult to conceal. This paper aims to evaluate the novel minimally invasive technique of robotic-assisted surgery.
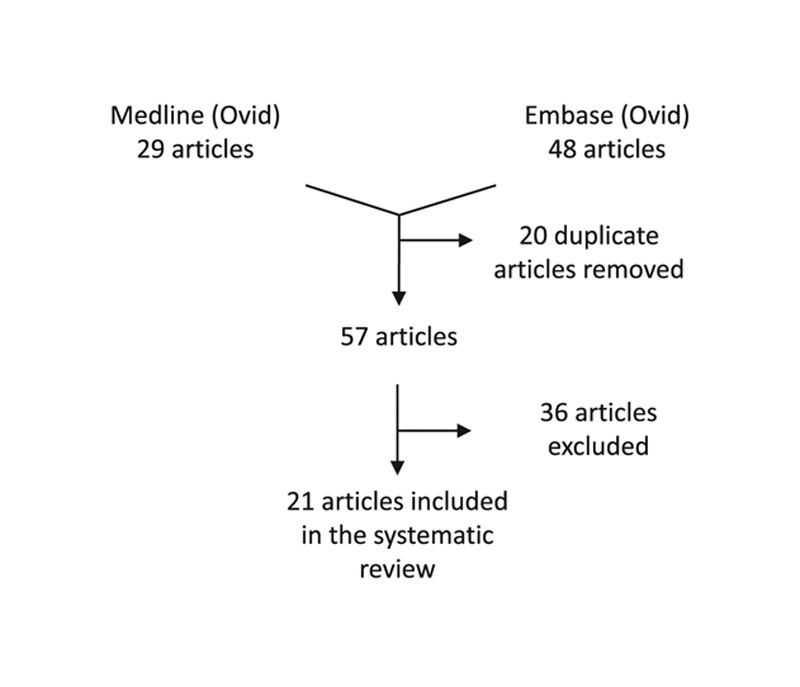
Methods: A systematic review was conducted using Medline (OvidSP) and Embase (OvidSP) to evaluate the current application of robotic-assisted surgery in breast surgery and reconstruction.
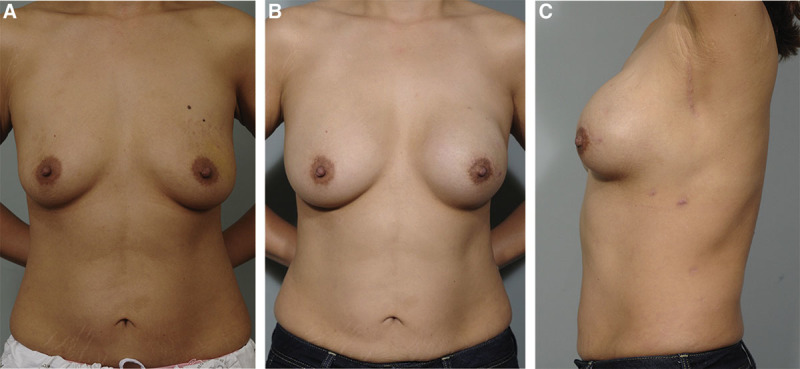
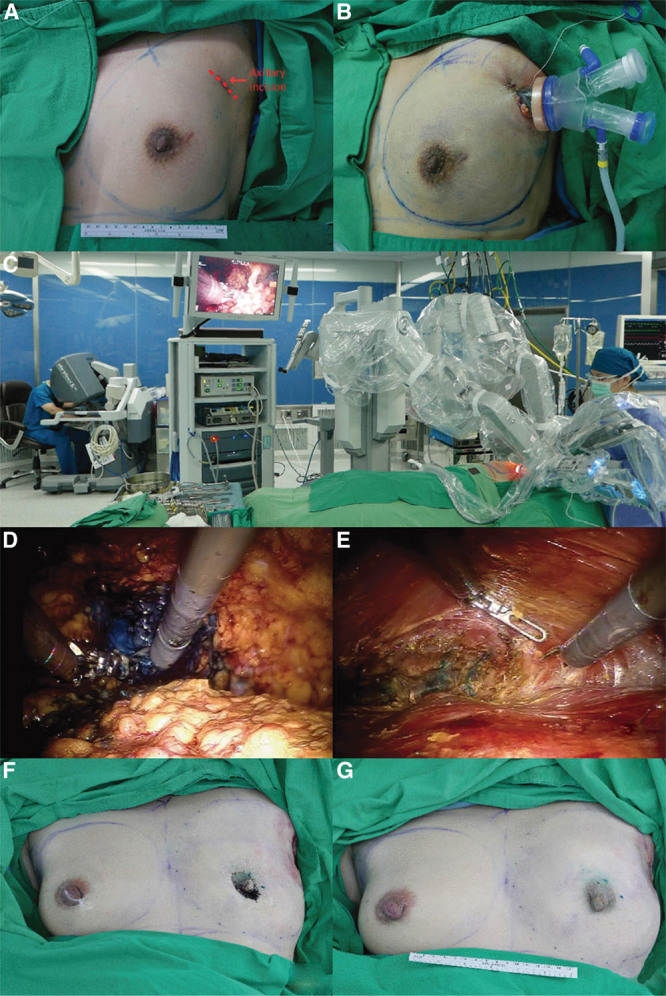
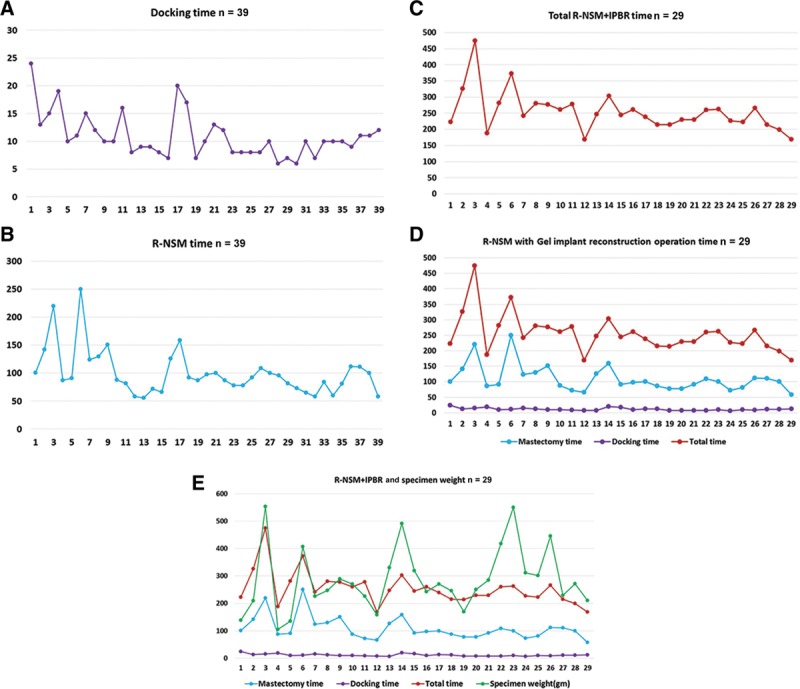
Results: Twenty-one articles were identified and discussed, composing of level 4 and 5 evidence comparing different surgeons' experiences, techniques, and outcomes. To date, the robotic system has been utilized to harvest the latissimus dorsi muscle for use as a tissue flap (total harvest time of 92 minutes), to perform nipple-sparing mastectomy with immediate breast reconstruction (total operation time 85 minutes) and lately to harvest a deep inferior epigastric perforator flap via an intraabdominal approach.
Conclusions: Robotic-assisted surgery can successfully and reproducibly perform a nipple-sparing mastectomy with breast reconstruction. It can minimize the size of scarring and is superior to the laparoscopic technique, with improved 3-dimensional visualization, dexterity, and range of motion able to guide around the curvature of the breast. The main limiting factors are the lack of the US Food and Drug Administration approval, cost of the robot, and specialized skills required.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
Figures

References
-
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Cancer Research UK. Breast cancer statistics. https://www.cancerresearchuk.org/health-professional/cancer-statistics/s.... Accessed December 29, 2018.
-
- Jamison KR, Wellisch DK, Pasnau RO. Psychosocial aspects of mastectomy: I. The women’s perspective. Am J Psychiatry. 1978;135:432–436. - PubMed
-
- Markopoulos C, Tsaroucha AK, Kouskos E, et al. Impact of breast cancer surgery on the self-esteem and sexual life of female patients. J Int Med Res. 2009;37:182–188. - PubMed
-
- Chen W, Lv X, Xu X, et al. Meta-analysis for psychological impact of breast reconstruction in patients with breast cancer. Breast Cancer. 2018;25:464–469. - PubMed
LinkOut - more resources
Full Text Sources