

Elevated incidence of alveolar echinococcosis in immunocompromised patients
- PMID: 32095630
- PMCID: PMC7034048
- DOI: 10.1016/j.fawpar.2019.e00060
Elevated incidence of alveolar echinococcosis in immunocompromised patients
Erratum in
-
Erratum regarding missing Declaration of Competing Interest statements in previously published articles.Food Waterborne Parasitol. 2020 Dec 15;21:e00105. doi: 10.1016/j.fawpar.2020.e00105. eCollection 2020 Dec. Food Waterborne Parasitol. 2020. PMID: 33385075 Free PMC article.
Abstract
Introduction: Recent experimental data has revealed that the course of alveolar echinococcosis (AE) depends on adaptive immunity. For this study, we aimed to analyze the incidence and outcome of AE in immunocompromised humans.
Material and methods: Retrospective analysis of 131 patients with a median age of 54 years treated for AE between 1971 and 2017 at a Swiss tertiary referral Centre. Fifty-two percent were females and 65 patients (50%) were diagnosed incidentally. Fourteen patients (16%) were operated on laparoscopically. Overall, median follow-up was 48 months.
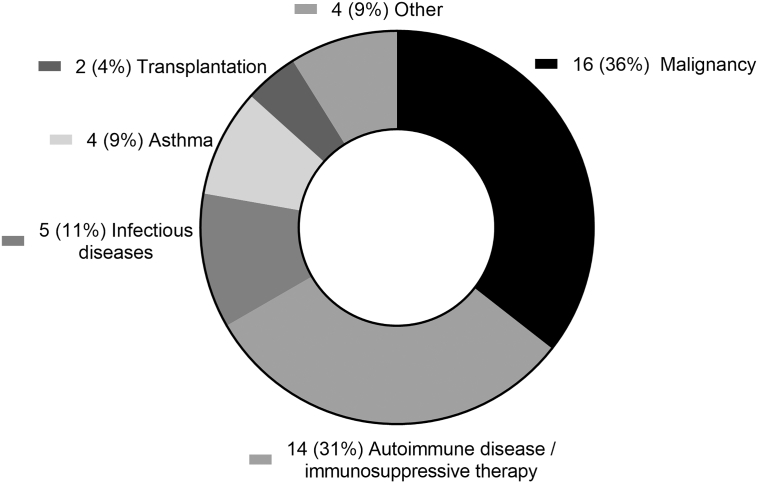
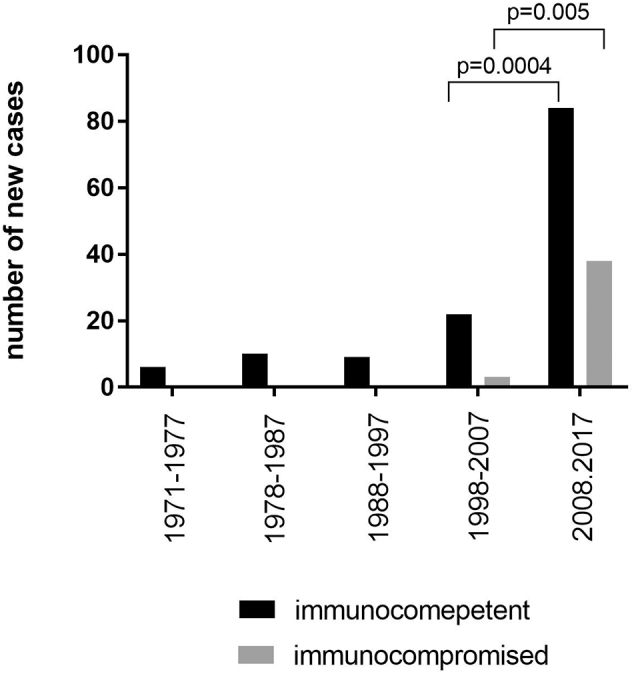
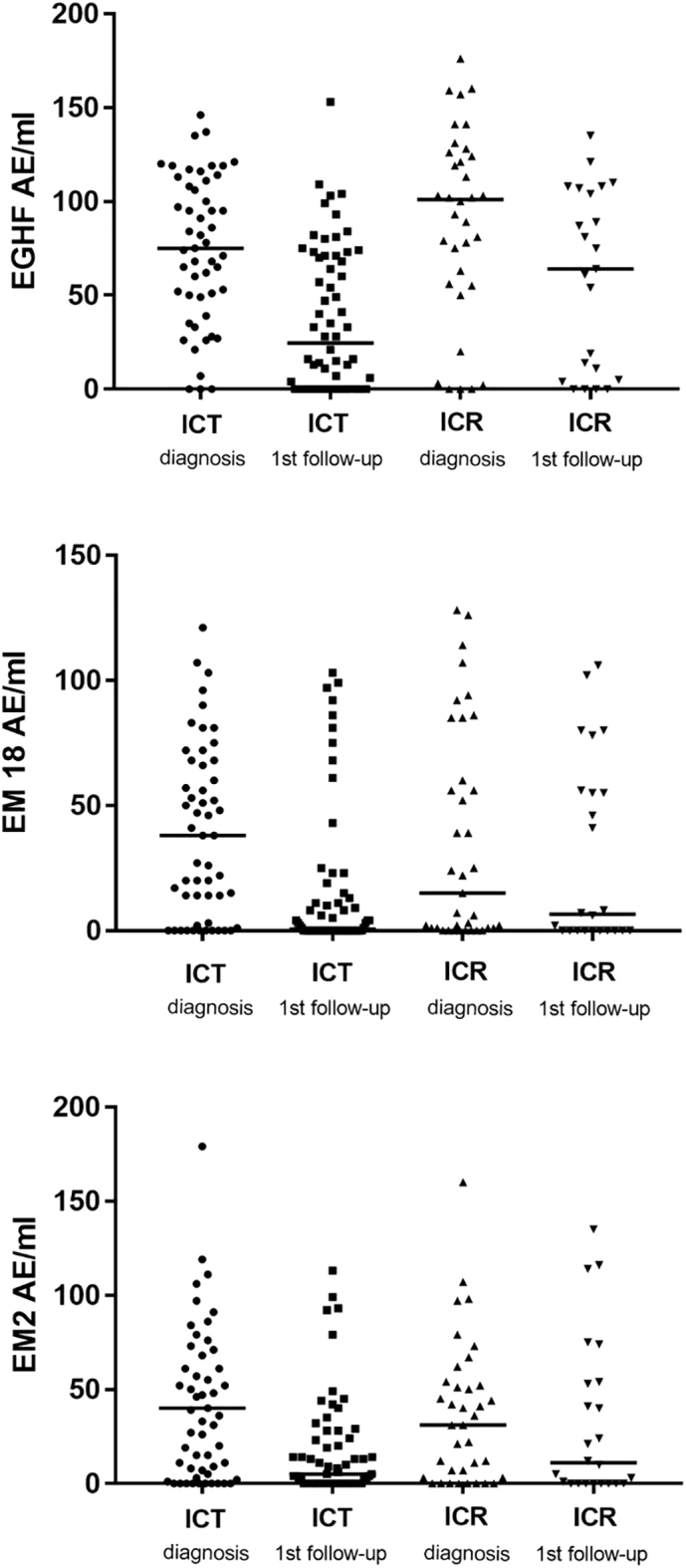
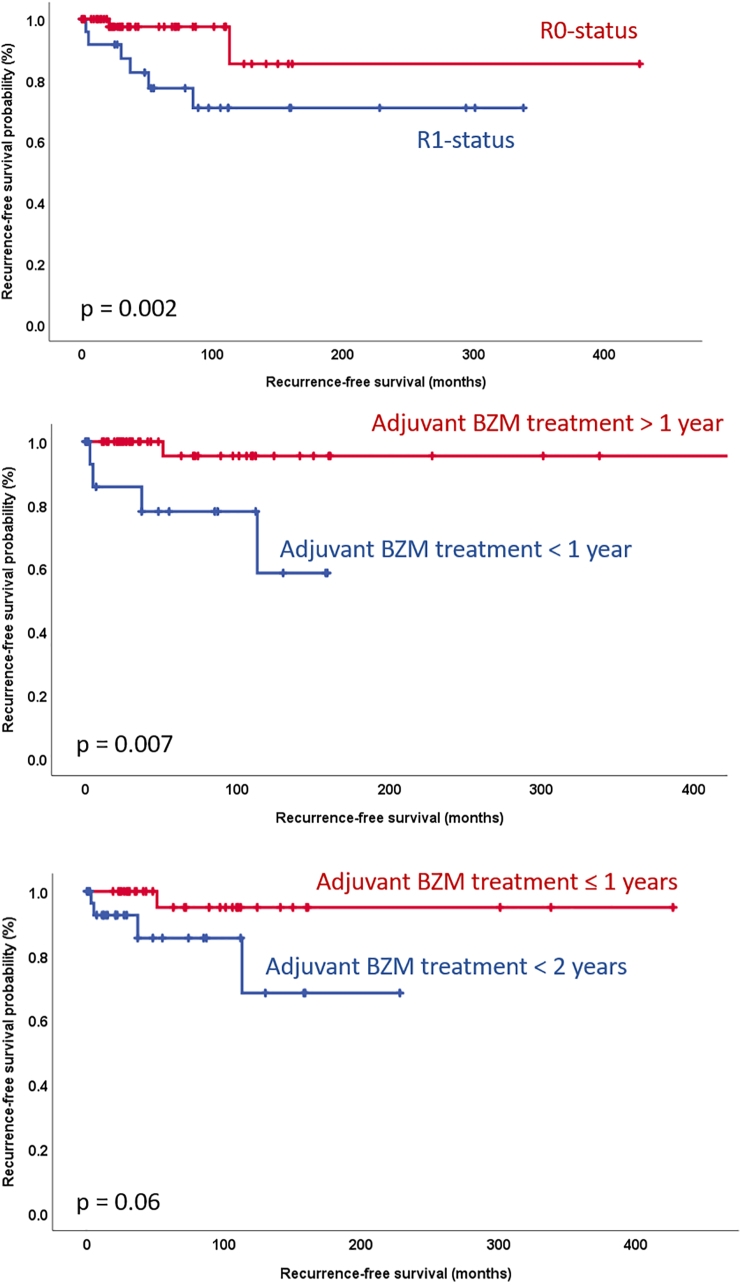
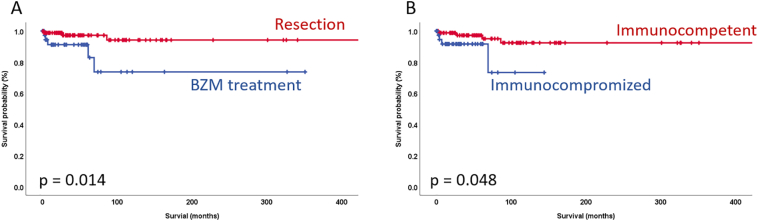
Results: New diagnoses have increased fourfold in immunocompetent and tenfold in immunocompromised patients in the past decade (p ≤ 0.005). Forty-one patients (31.3%) had co-existing or previous immunosuppressive conditions including 16 malignancies (36%), 11 auto-immune diseases or immunosuppressive therapies (31%), 5 infectious diseases (11%), 4 chronic asthma conditions (9%), 2 previous transplantations (4%) and 4 other immunocompromising conditions (9%). Serum levels of anti-Em18, -Em2 and -EgHF antibodies were neither associated with immunocompetence at diagnosis nor during follow-up, but significantly decreased after treatment with benzimidazole (n = 43) or surgery (n = 88) in all patients. Adjuvant therapy for ≥1 year (p = 0.007) with benzimidazole and resection status (R0) (p = 0.002) were both correlated with recurrence-free survival. Survival at 5 and 10 years after surgery was 97% and 94%, respectively, and after conservative treatment 91% and 73%, respectively. Curative surgery (p = 0.014) and immunocompetence (p = 0.048) correlated significantly with overall survival.
Conclusion: The incidence of human AE has increased over the last 2 decades with surgical interventions resulting in excellent outcomes. We have observed an association of immunosuppressive conditions with both incidence and survival of AE eventually justifying the implementation of a screening program for patients at risk in endemic regions.
Keywords: Alveolar echinococcosis, (AE); Benzimidazole; Echinoccocosis; Echinococcus multilocularis; Echinococcus multilocularis, (E. multilocularis); Immunosuppression; alveolar_echinococcosis; benzimidazole, (BZM); immunocompetent, (ICT); immunocompromised, (ICR).
© 2019 Published by Elsevier Inc. on behalf of International Association of Food and Waterborne Parasitology.
Figures
References
-
- Aji T., Dong J.H., Shao Y.M., Zhao J.M., Li T., Tuxun T., Shalayiadang P., Ran B., Jiang T.M., Zhang R.Q., He Y.B., Huang J.F., Wen H. Ex vivo liver resection and autotransplantation as alternative to allotransplantation for end-stage hepatic alveolar echinococcosis. J. Hepatol. 2018 - PubMed
-
- Allison A.C. Immunosuppressive drugs: the first 50 years and a glance forward. Immunopharmacology. 2000;47:63–83. - PubMed
-
- Beldi G., Vuitton D., Lachenmayer A., Heyd B., Dufour J.F., Richou C., Candinas D., Bresson-Hadni S. Is ex vivo liver resection and autotransplantation a valid alternative treatment for end-stage hepatic alveolar echinococcosis in Europe? J. Hepatol. 2019 - PubMed
-
- Bresson-Hadni S., Vuitton D.A., Bartholomot B., Heyd B., Godart D., Meyer J.P., Hrusovsky S., Becker M.C., Mantion G., Lenys D., Miguet J.P. A twenty-year history of alveolar echinococcosis: analysis of a series of 117 patients from eastern France. Eur. J. Gastroenterol. Hepatol. 2000;12:327–336. - PubMed
-
- Brunetti E., Kern P., Vuitton D.A., Writing Panel for the, W.-I Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010;114:1–16. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
