

False lumen embolization as a rescue technique in the setting of acute and chronic dissecting aneurysms as adjunct to thoracic endovascular aortic repair
- PMID: 32095669
- PMCID: PMC7033463
- DOI: 10.1016/j.jvscit.2019.12.004
False lumen embolization as a rescue technique in the setting of acute and chronic dissecting aneurysms as adjunct to thoracic endovascular aortic repair
Abstract
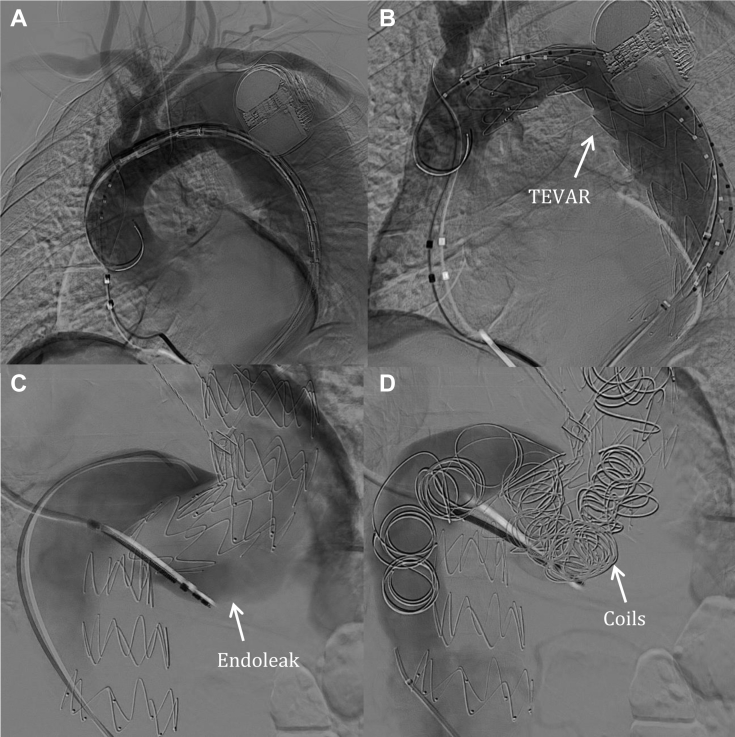
Complicated type B aortic dissection (TBAD) is a life-threatening condition requiring surgical intervention. One such complication in the acute or chronic setting is aneurysmal degeneration. The dissected aortic wall is weakened, and the pressures in the false lumen are often high. In the past decade, thoracic endovascular aortic repair (TEVAR) has become the treatment of choice for TBAD. TEVAR can be complicated by lack of false lumen thrombosis, increasing the risk of death. We present three cases of TBAD with patent false lumens after TEVAR that were treated by false lumen coil embolization.
Keywords: Aortic dissection; Coil embolization; Dissecting aortic aneurysm; Endovascular; False lumen; TEVAR.
© 2020 The Authors.
Figures








References
-
- Nauta F.J., Trimarchi S., Kamman A.V., Moll F.L., van Herwaarden J.A., Patel H.J. Update in the management of type B aortic dissection. Vasc Med. 2016;21:251–263. - PubMed
-
- Qin Y.L., Deng G., Li T.X., Wang W., Teng G.J. Treatment of acute type-B aortic dissection: thoracic endovascular aortic repair or medical management alone? JACC Cardiovasc Interv. 2013;6:185–191. - PubMed
-
- Sumpio B.J., Cordova A.D., Mahler D., Sumpio B.E. Use of negative pressure wound therapy in healing below knee amputation in patients with chronic venous insufficiency and/or Charcot disease. Angiology Open Access. 2013;1:1000112.
-
- Ruddy J.M., Reisenman P., Priestley J., Brewster L.P., Duwayri Y., Veeraswamy R.K. Stent graft therapy for false lumen aneurysmal degeneration in established type B aortic dissection (FADED) results in differential volumetric remodeling of the thoracic versus abdominal aortic segments. Ann Vasc Surg. 2014;28:1602–1609. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
