

Association between mortality rates and medication and residential treatment after in-patient medically managed opioid withdrawal: a cohort analysis
- PMID: 32096908
- PMCID: PMC7854020
- DOI: 10.1111/add.14964
Association between mortality rates and medication and residential treatment after in-patient medically managed opioid withdrawal: a cohort analysis
Abstract
Background and aim: Medically managed opioid withdrawal (detox) can increase the risk of subsequent opioid overdose. We assessed the association between mortality following detox and receipt of medications for opioid use disorder (MOUD) and residential treatment after detox.
Design: Cohort study generated from individually linked public health data sets.
Setting: Massachusetts, USA.
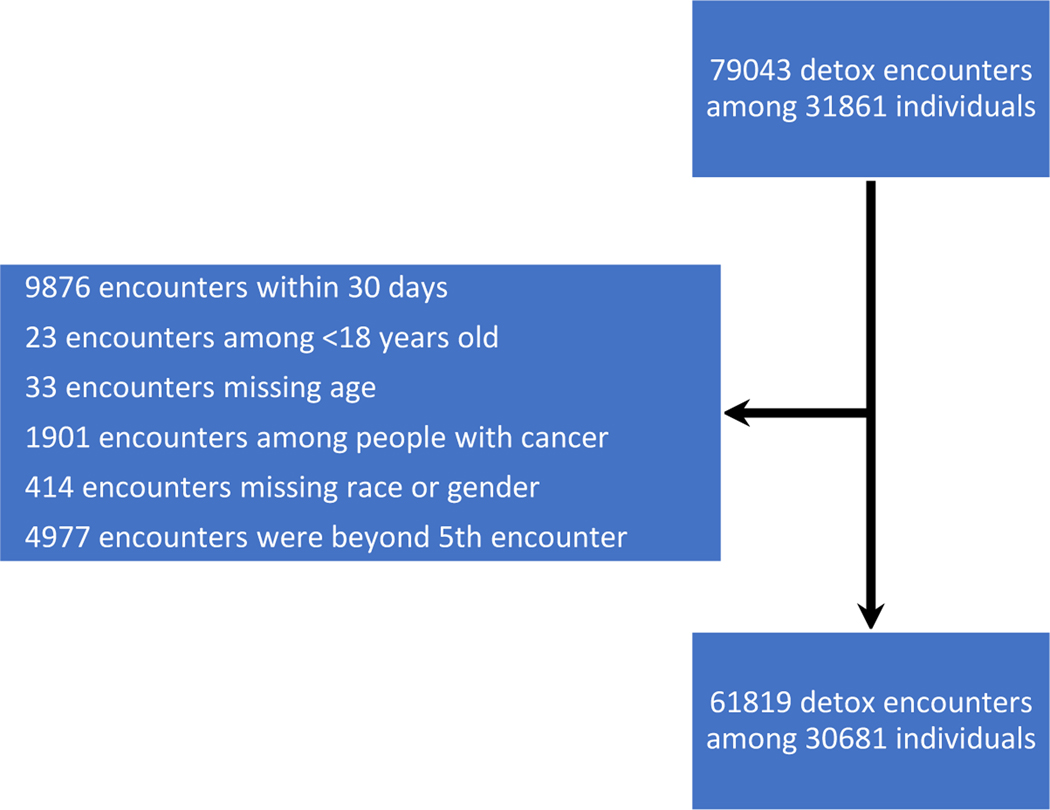
Participants: A total of 30 681 opioid detox patients with 61 819 detox episodes between 2012 and 2014.
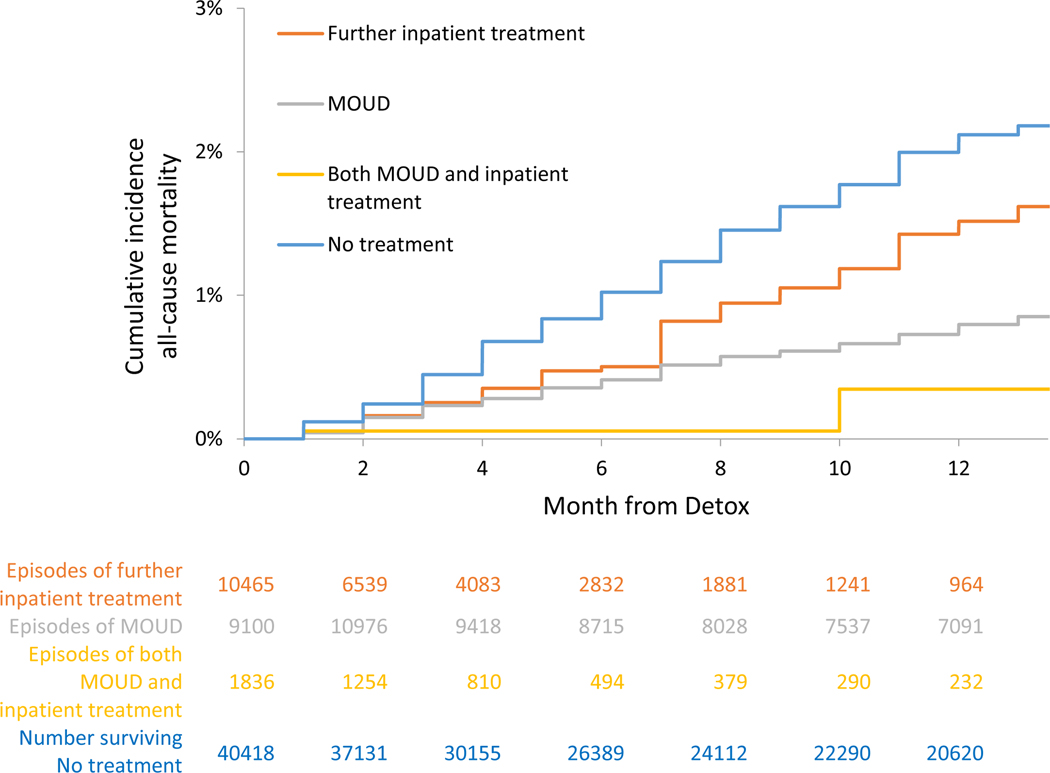
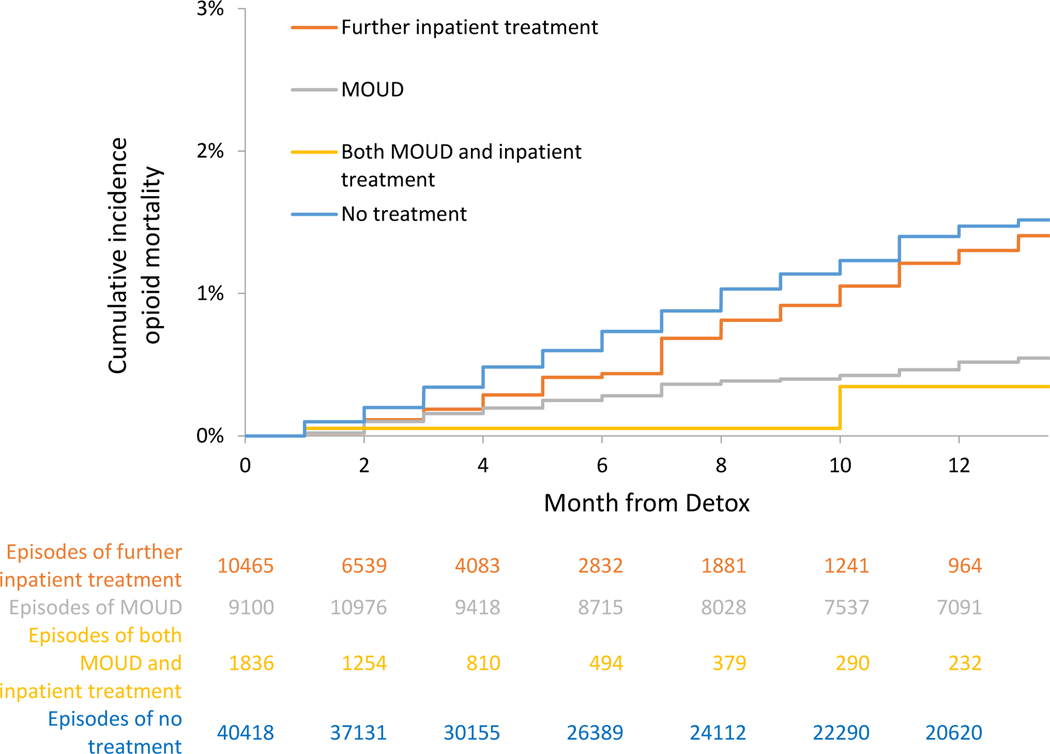
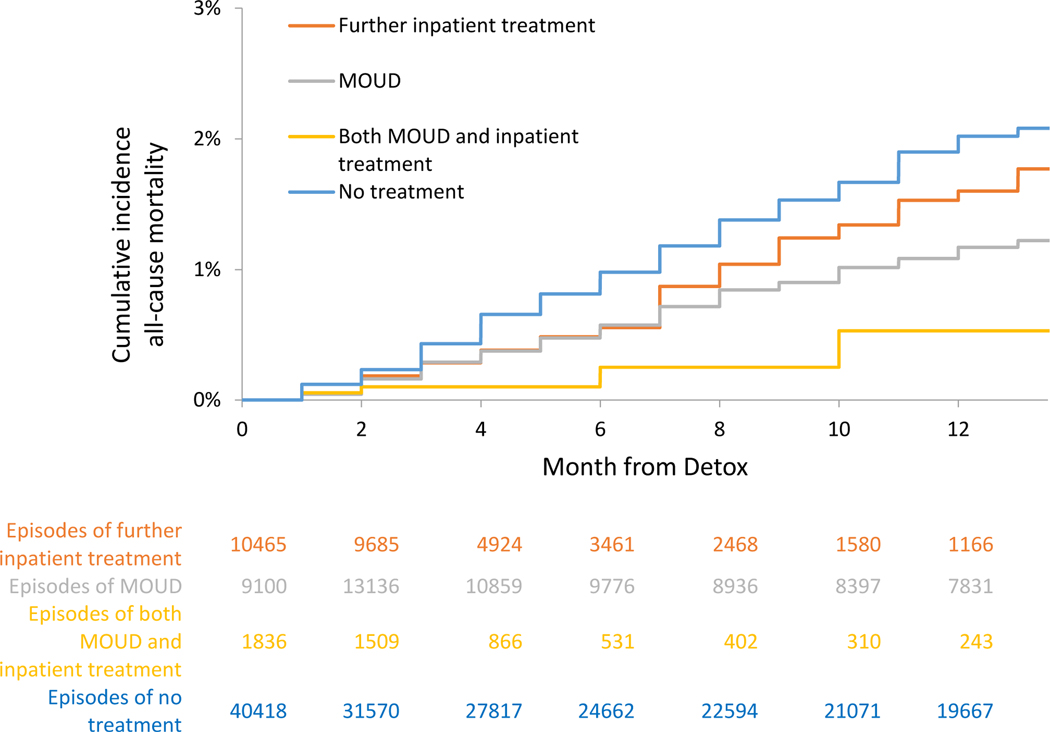
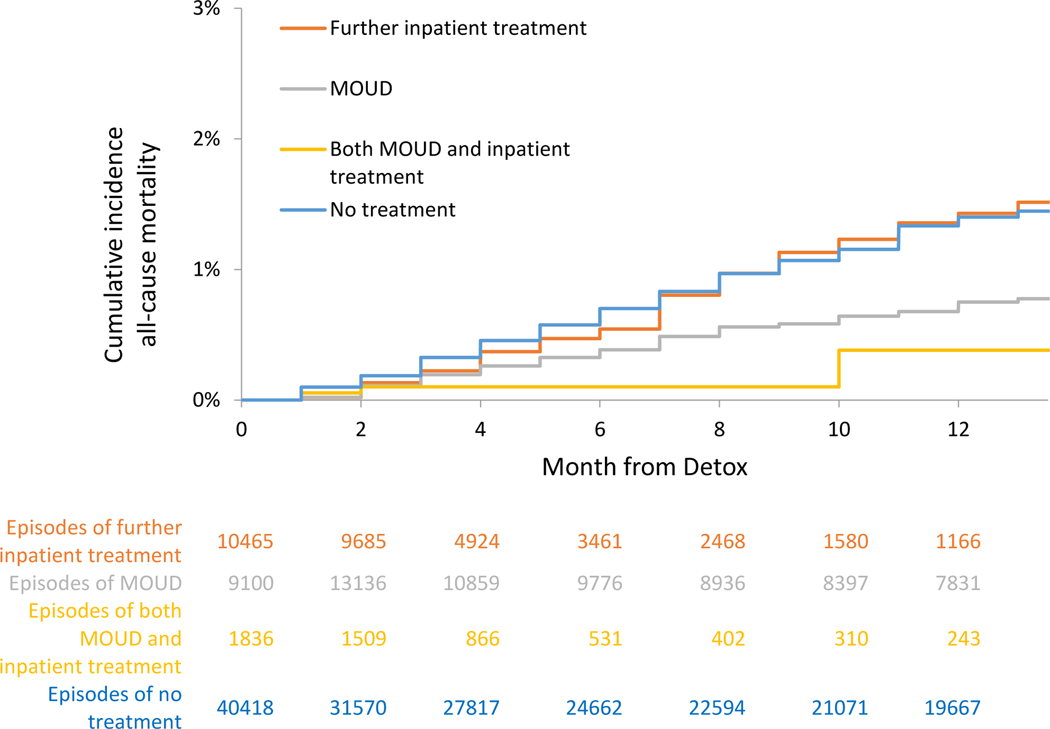
Measurements: Treatment categories included no post-detox treatment, MOUD, residential treatment or both MOUD and residential treatment identified at monthly intervals. We classified treatment exposures in two ways: (a) 'on-treatment' included any month where a treatment was received and (b) 'with-discontinuation' individuals were considered exposed through the month following treatment discontinuation. We conducted multivariable Cox proportional hazards analyses and extended Kaplan-Meier estimator cumulative incidence for all-cause and opioid-related mortality for the treatment categories as monthly time-varying exposure variables.
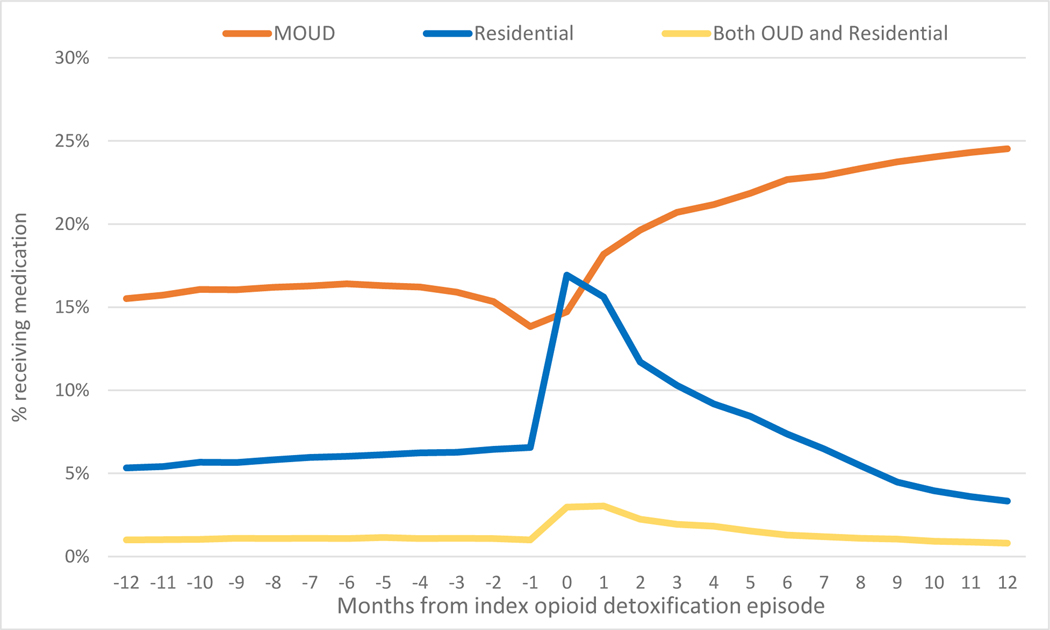
Findings: Twelve months after detox, 41% received MOUD for a median of 3 months, 35% received residential treatment for a median of 2 months and 13% received both for a median of 5 months. In on-treatment analyses for all-cause mortality compared with no treatment, adjusted hazard ratios (AHR) were 0.34 [95% confidence interval (CI) = 0.27-0.43] for MOUD, 0.63 (95% CI = 0.47-0.84) for residential treatment and 0.11 (95% CI = 0.03-0.43) for both. In with-discontinuation analyses for all-cause mortality, compared with no treatment, AHRs were 0.52 (95% CI = 0.42-0.63) for MOUD, 0.76 (95% CI = 0.59-0.96) for residential treatment and 0.21 (95% CI = 0.08-0.55) for both. Results were similar for opioid-related overdose mortality.
Conclusions: Among people who have undergone medically managed opioid withdrawal, receipt of medications for opioid use disorder, residential treatment or the combination of medications for opioid use disorder and residential treatment were associated with substantially reduced mortality compared with no treatment.
Keywords: Detox; medically managed withdrawal; medication for opioid use disorders; mortality; overdose; residential treatment.
© 2020 Society for the Study of Addiction.
Conflict of interest statement
Figures
Similar articles
-
Medication for Opioid Use Disorder After Nonfatal Opioid Overdose and Association With Mortality: A Cohort Study.Ann Intern Med. 2018 Aug 7;169(3):137-145. doi: 10.7326/M17-3107. Epub 2018 Jun 19. Ann Intern Med. 2018. PMID: 29913516 Free PMC article.
-
Characteristics and Receipt of Medication Treatment Among Young Adults Who Experience a Nonfatal Opioid-Related Overdose.Ann Emerg Med. 2020 Jan;75(1):29-38. doi: 10.1016/j.annemergmed.2019.07.030. Epub 2019 Oct 4. Ann Emerg Med. 2020. PMID: 31591014 Free PMC article.
-
Population-level impact of initiating pharmacotherapy and linking to care people with opioid use disorder at inpatient medically managed withdrawal programs: an effectiveness and cost-effectiveness analysis.Addiction. 2022 Sep;117(9):2450-2461. doi: 10.1111/add.15879. Epub 2022 Apr 12. Addiction. 2022. PMID: 35315162 Free PMC article.
-
Adherence to and Retention in Medications for Opioid Use Disorder Among Adolescents and Young Adults.Epidemiol Rev. 2020 Jan 31;42(1):41-56. doi: 10.1093/epirev/mxaa001. Epidemiol Rev. 2020. PMID: 32239206 Free PMC article.
-
Access to Medications for Opioid Use Disorder and Associated Factors Among Adolescents and Young Adults: A Systematic Review.JAMA Pediatr. 2022 Mar 1;176(3):304-311. doi: 10.1001/jamapediatrics.2021.4606. JAMA Pediatr. 2022. PMID: 34870707 Free PMC article.
Cited by
-
Drug Overdose Death Following Substance Use Disorder Treatment Termination in New York City: A Retrospective Longitudinal Cohort Study.J Urban Health. 2024 Oct;101(5):1045-1057. doi: 10.1007/s11524-024-00893-5. Epub 2024 Aug 2. J Urban Health. 2024. PMID: 39095494
-
Surmounting Withdrawal to Initiate Fast Treatment with Naltrexone (SWIFT): A stepped wedge hybrid type 1 effectiveness-implementation study.Contemp Clin Trials. 2023 May;128:107148. doi: 10.1016/j.cct.2023.107148. Epub 2023 Mar 15. Contemp Clin Trials. 2023. PMID: 36931426 Free PMC article. Clinical Trial.
-
Association of facility characteristics and substance use disorder outcomes at discharge from residential treatment.J Subst Abuse Treat. 2022 May;136:108664. doi: 10.1016/j.jsat.2021.108664. Epub 2021 Nov 15. J Subst Abuse Treat. 2022. PMID: 34840041 Free PMC article.
-
An Approach to Enhancing Medication Treatment for Opioid Use Disorder in the HEALing Communities Study.Psychiatr Serv. 2024 Jun 1;75(6):580-588. doi: 10.1176/appi.ps.20230159. Epub 2024 Feb 13. Psychiatr Serv. 2024. PMID: 38347814 Free PMC article.
-
Escalating Doses of Buprenorphine for the Treatment of Buprenorphine-Induced Opioid Withdrawal.Cureus. 2025 Mar 13;17(3):e80527. doi: 10.7759/cureus.80527. eCollection 2025 Mar. Cureus. 2025. PMID: 40225488 Free PMC article.
References
-
- Degenhardt L, Bucello C, Mathers B, Briegleb C, Ali H, Hickman M, et al. Mortality among regular or dependent users of heroin and other opioids: a systematic review and meta-analysis of cohort studies. Addiction. 2011. January;106(1):32–51. - PubMed
-
- Mee-Lee D, Shulman GD, Fishman MJ, Gastfriend D, Miller MM, Provence SM. The ASAM Criteria: Treatment Criteria for Addictive, Substance-Related, and Co-Occuring Conditions [Internet]. The Change Companies; 2013. [cited 2019 Apr 1]. Available from: https://www.americanhealthholding.com/Content/Pdfs/asam%20criteria.pdf
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
