

Multidimensional tracking of phenotypes and organ involvement in a complete nationwide systemic sclerosis cohort
- PMID: 32097470
- PMCID: PMC7516103
- DOI: 10.1093/rheumatology/keaa026
Multidimensional tracking of phenotypes and organ involvement in a complete nationwide systemic sclerosis cohort
Abstract
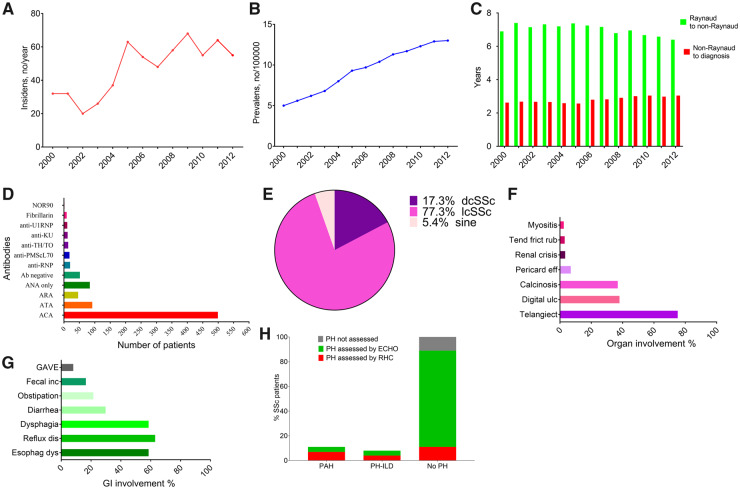
Objective: SSc is a severe, heterogeneous multi-organ disease where population-based estimates on phenotypic spectrum, overall disease burden and societal impact are largely missing. Here the objective was to provide the first-ever complete national-level data on phenotype and major organ afflictions in SSc.
Methods: A stepwise strategy was applied to find and characterize every SSc patient resident in Norway from 2000 to 2012. First we identified every case in the country registered with an International Classification of Diseases, Tenth Revision code for SSc (M34). Next we manually reviewed all cases coded as M34 to determine whether they met the 1980 ACR and/or 2013 ACR/EULAR classification criteria for SSc and could be included in the Norwegian SSc cohort (Nor-SSc). Finally, all disease features from SSc onset to study end were reviewed.
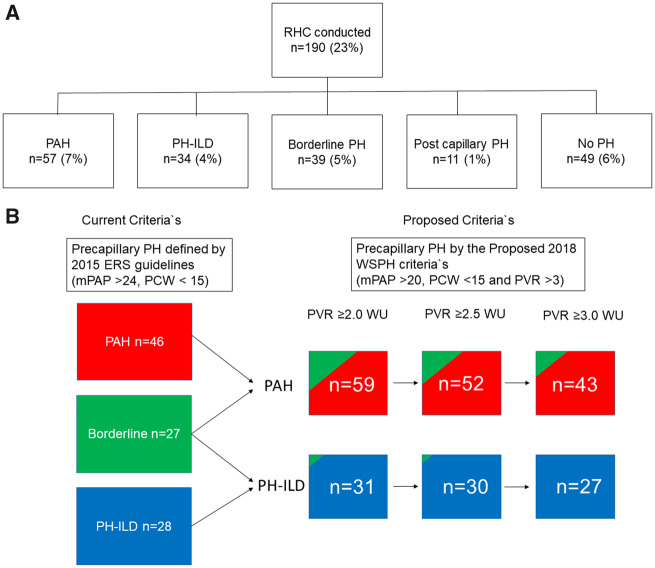
Results: The Nor-SSc cohort included 815 SSc patients. The mean age at diagnosis was 53 years, with 84% females and 77% limited cutaneous SSc. The estimated incidence increased from 4 per million in 2000 to 13 per million in 2012. We identified high cumulative frequencies of internal organ involvement, coexistence of multiple organ afflictions across disease subsets and autoantibody status and stable frequencies of pulmonary arterial hypertension across haemodynamic definitions, but indications of referral-related differences in pulmonary hypertension detection rates across the study area.
Conclusion: This nationwide cohort study provides new, unbiased evidence for a high disease burden in SSc patients of Caucasian descent and indicates the existence of hurdles preventing equality of assessment across the SSc population.
Keywords: epidemiology; gastrointestinal involvement; interstitial lung disease; pulmonary hypertension; systemic sclerosis.
© The Author(s) 2020. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures


References
-
- Allanore Y, Denton C, Matucci-Cerinic M.. Systemic sclerosis In: Bijlsma JWJ, ed. EULAR Textbook on Rheumatic Diseases. Kilchberg, Switzerland: European League Against Rheumatism, 2012.
-
- Denton CP, Khanna D.. Systemic sclerosis. Lancet 2017;390:1685–99. - PubMed
-
- Nihtyanova S, Schreiber B, Ong V. et al. Prediction of pulmonary complications and long-term survival in systemic sclerosis. Arthritis Rheumatol 2014;66:1625–35. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
