

Relationship of Nocturnal Wakefulness to Suicide Risk Across Months and Methods of Suicide
- PMID: 32097547
- PMCID: PMC8121668
- DOI: 10.4088/JCP.19m12964
Relationship of Nocturnal Wakefulness to Suicide Risk Across Months and Methods of Suicide
Abstract
Objective: Insomnia is a risk factor for suicide, and the risk of suicide after accounting for population wakefulness is disproportionately highest at night. This study investigated whether this risk varied across months and/or methods of suicide.
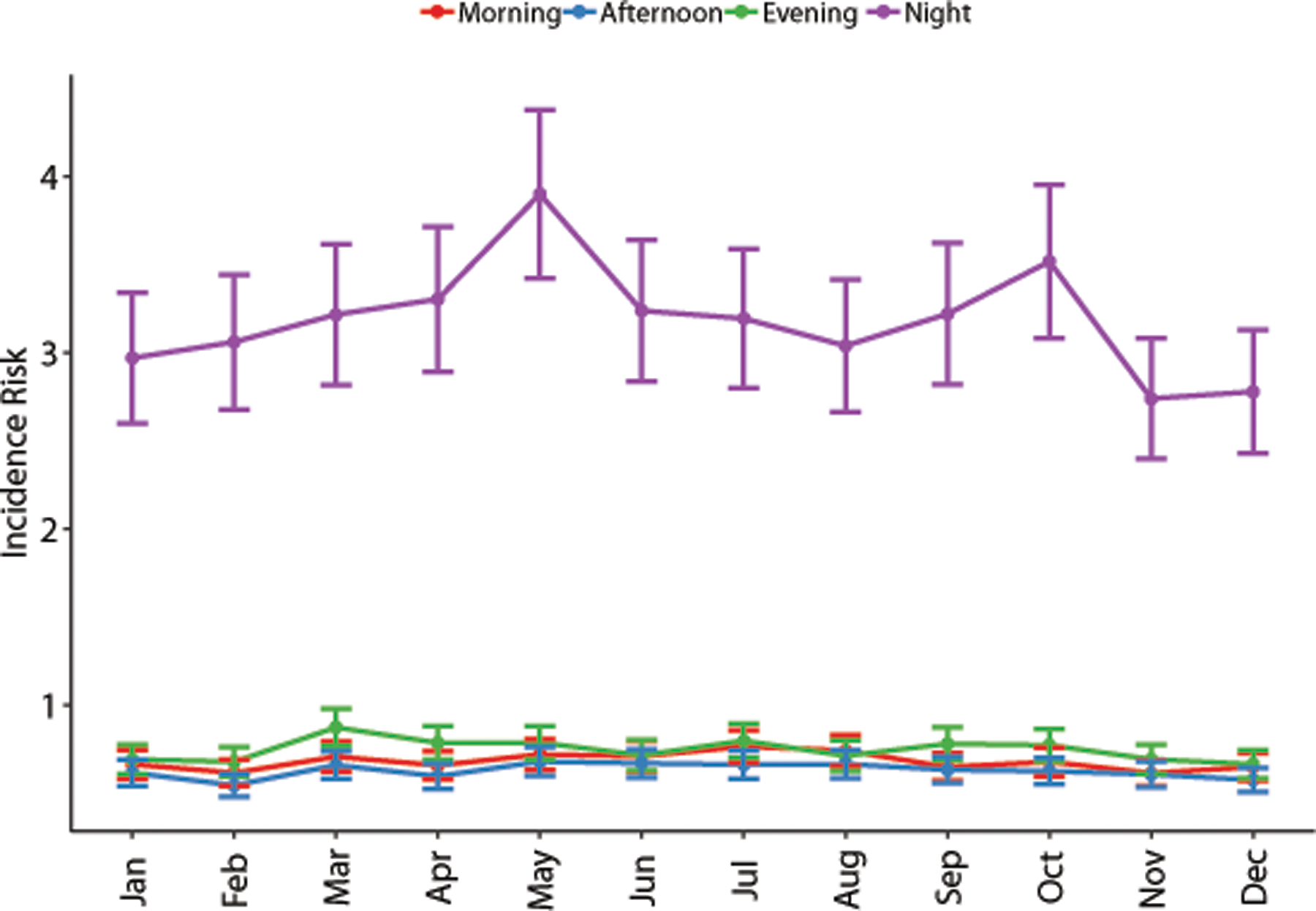
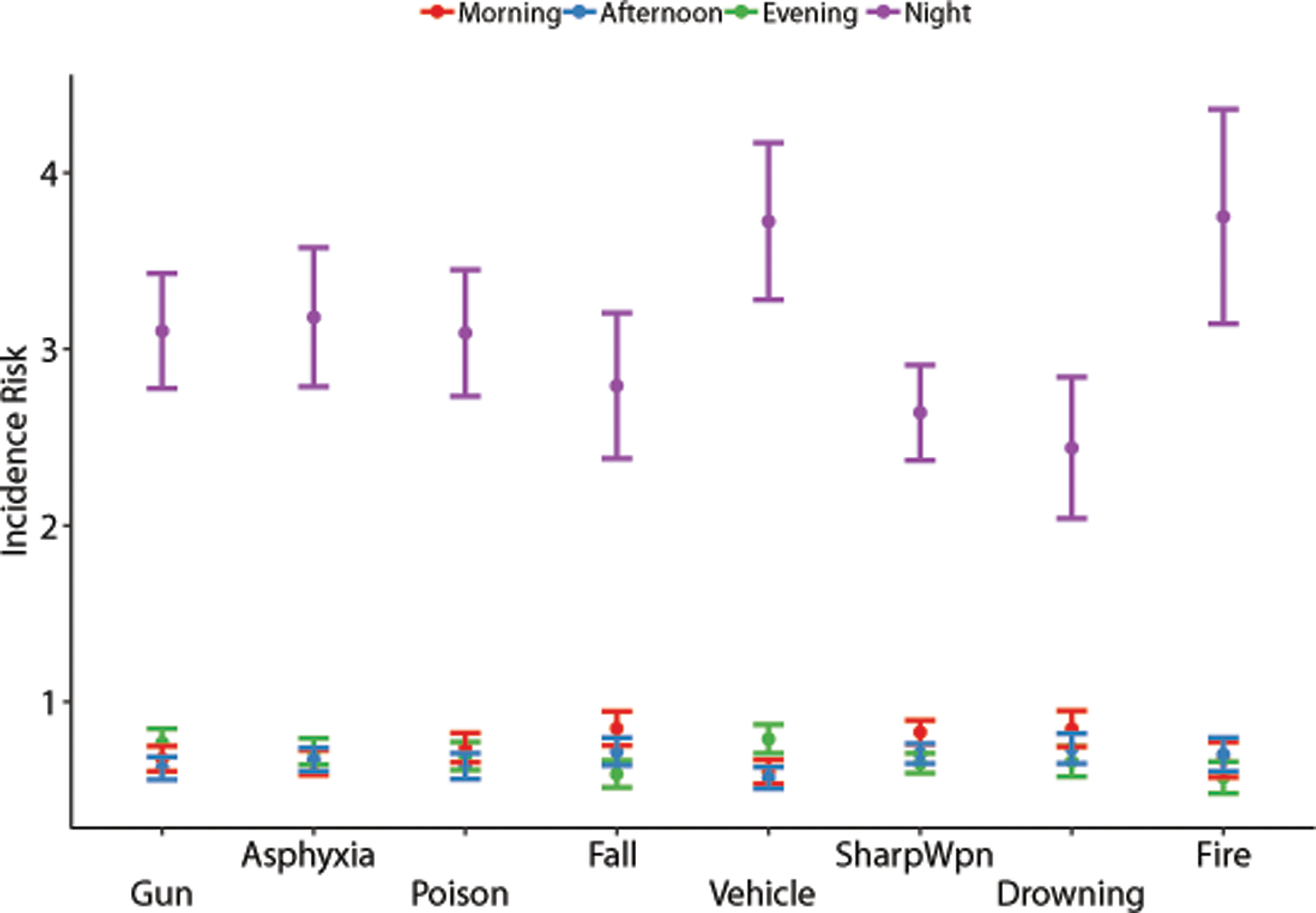
Methods: Time, date, method (eg, firearm, poisoning), and demographic information for 35,338 suicides were collected from the National Violent Death Reporting System for the years 2003-2010. Time of fatal injury was grouped into 1-hour bins and compared to the estimated hourly proportion of the population awake from the American Time Use Survey for 2003-2010. Negative binomial modeling then generated hourly incidence risk ratios (IRRs) of suicide. Risks were then aggregated into 4 categories: morning (6:00 am to 11:59 am), afternoon (noon to 5:59 pm), evening (6:00 pm to 11:59 pm), and night (midnight to 5:59 am).
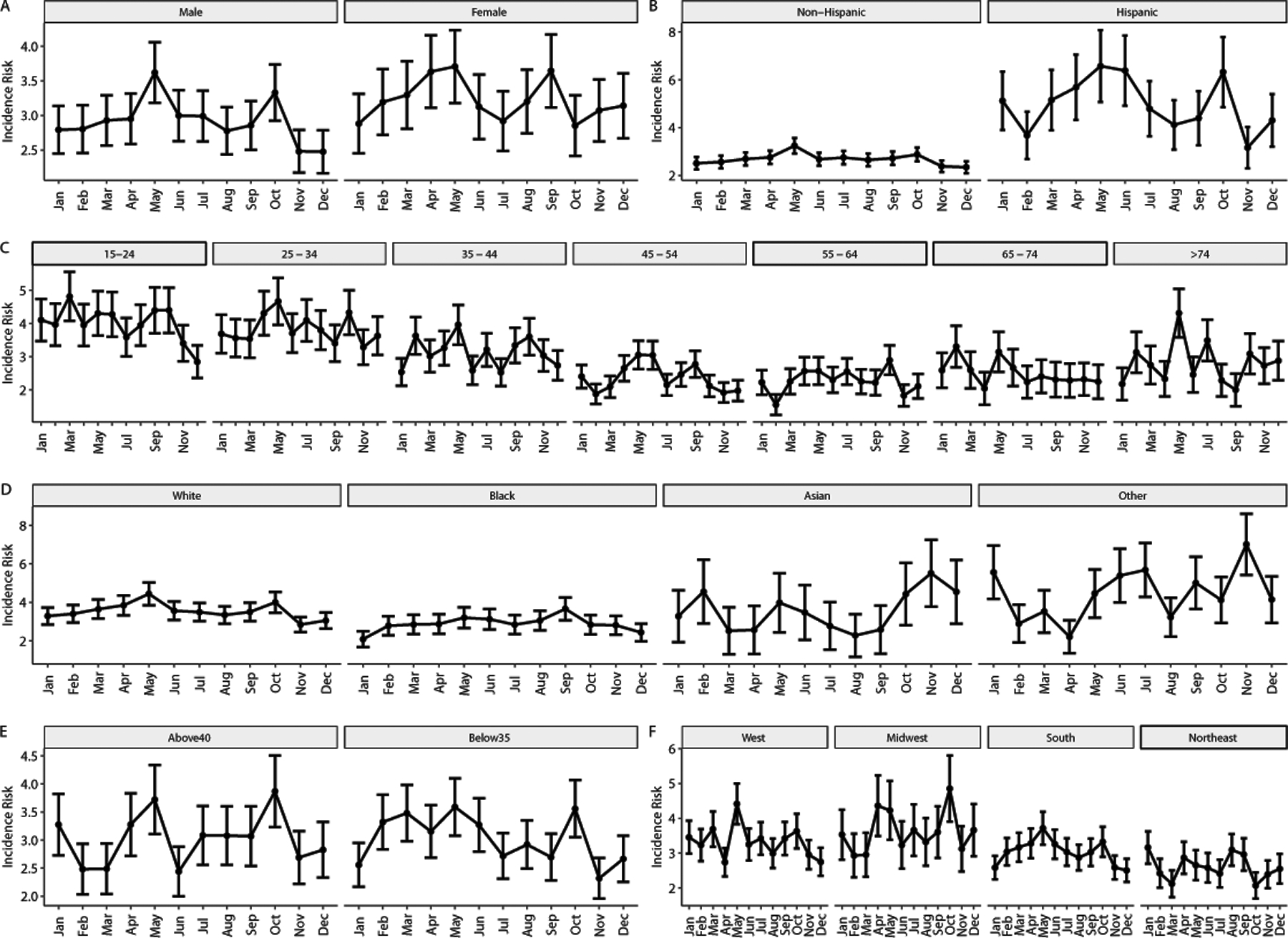
Results: The risk of suicide was higher at night across all months (P < .001) and methods (P < .001). The mean nocturnal IRR across months was 3.18 (SD = 0.314), with the highest IRR in May (3.90) and the lowest in November (2.74). The mean (SD) nocturnal IRR across methods was 3.09 (0.472), with the highest IRR for fire (3.75) and the lowest for drowning (2.44). Additionally, nocturnal risk was elevated within all demographics (all P < .001). However, there were no month-by-time or method-by-time interactions across demographics (all P > .05).
Conclusions: Regardless of month or method, the incidence risk of suicide at night is higher than at any other time of day. Additionally, demographic subgroups did not differentially experience higher risks across months or mechanisms at night.
© Copyright 2020 Physicians Postgraduate Press, Inc.
Conflict of interest statement
Conflicts of interest: none.
Figures

References
-
- Pigeon WR, Pinquart M, Conner K. Meta-analysis of sleep disturbance and suicidal thoughts and behaviors. J Clin Psychiatry. 2012;73(9):e1160–1167. - PubMed
-
- Bozzay ML, Karver MS, Verona E. Linking insomnia and suicide ideation in college females: The role of socio-cognitive variables and depressive symptoms in suicide risk. J Affect Disord. 2016;199:106–113. - PubMed
-
- Nadorff MR, Anestis MD, Nazem S, Claire Harris H, Samuel Winer E. Sleep disorders and the interpersonal-psychological theory of suicide: independent pathways to suicidality? J Affect Disord. 2014;152–154:505–512. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
