

Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature
- PMID: 32098249
- PMCID: PMC7073116
- DOI: 10.3390/ijms21041483
Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature
Abstract
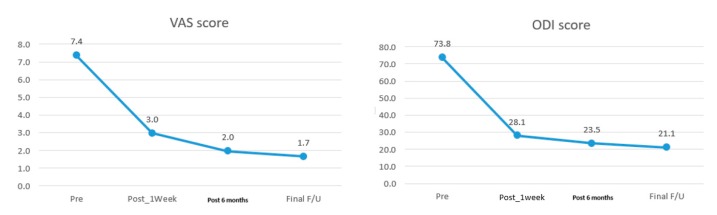
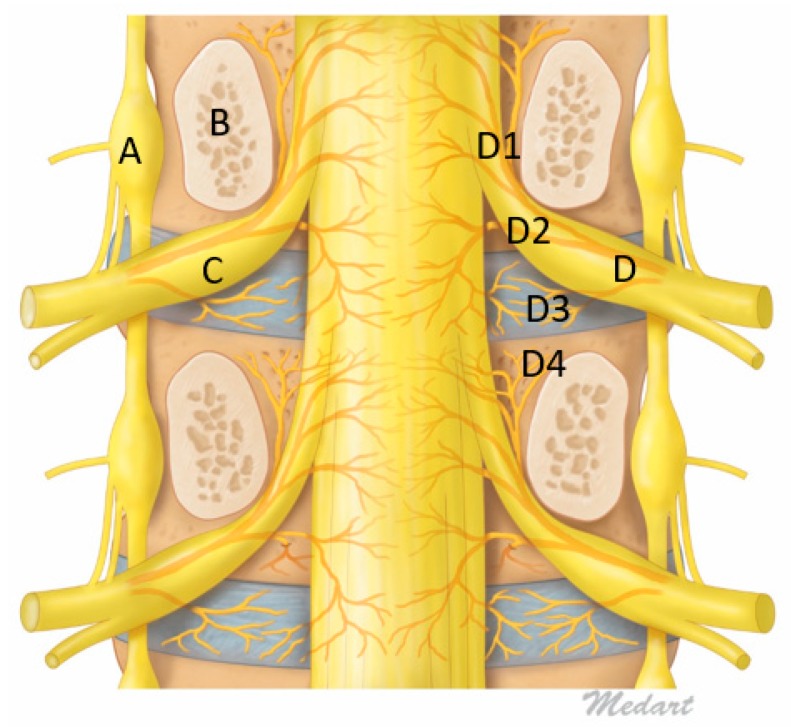
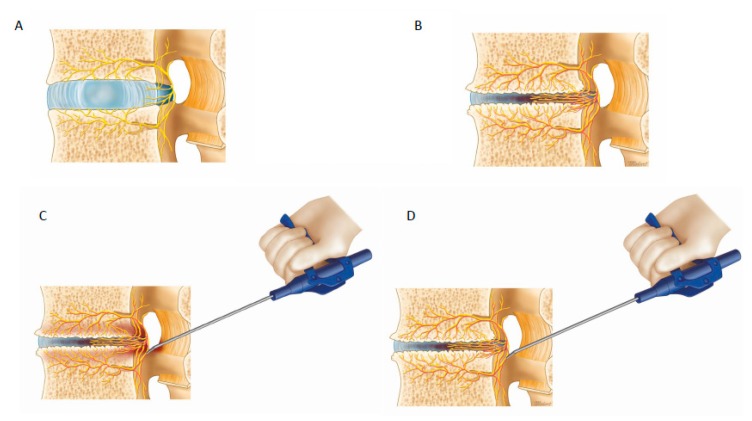
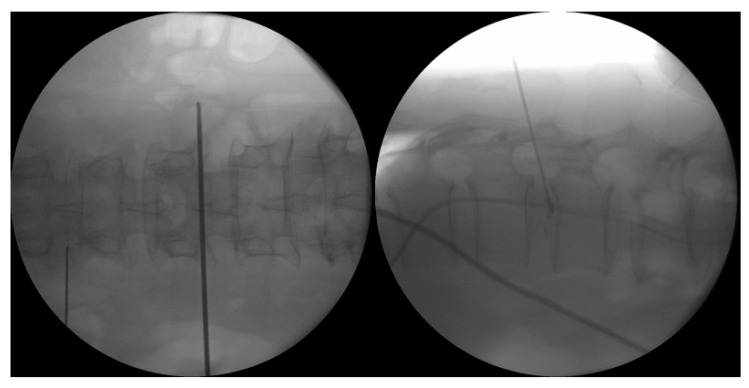
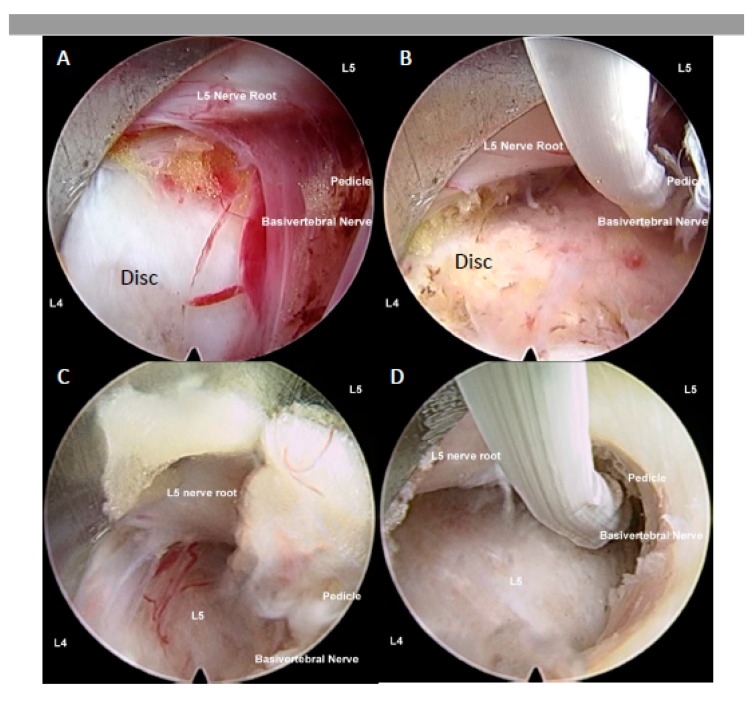
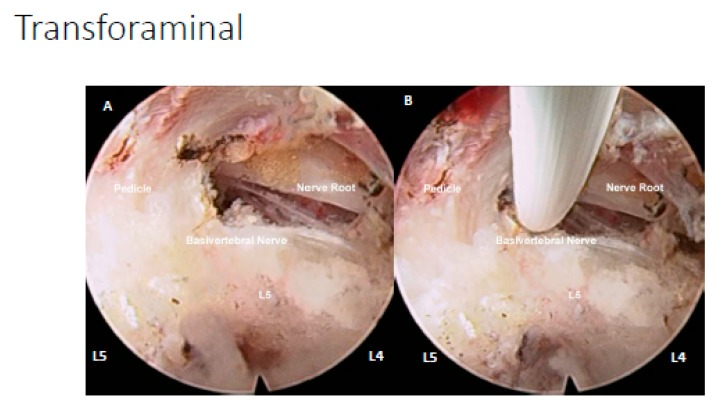
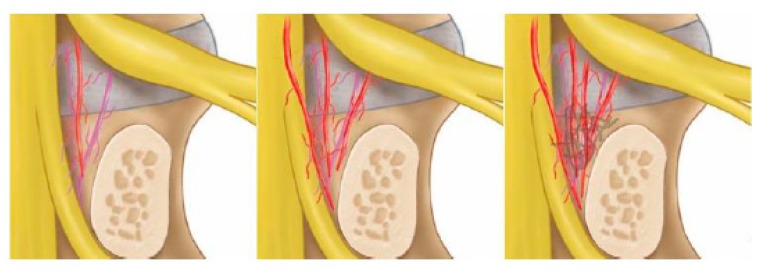
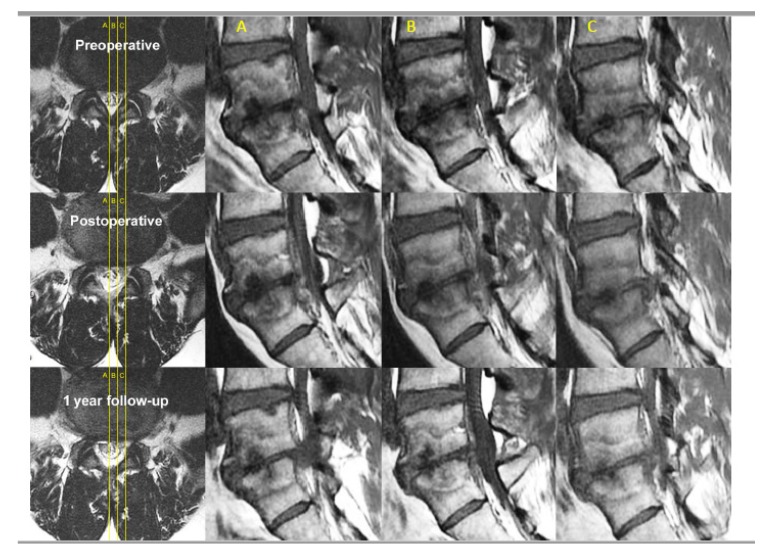
Degenerative disc disease is a leading cause of chronic back pain in the aging population in the world. Sinuvertebral nerve and basivertebral nerve are postulated to be associated with the pain pathway as a result of neurotization. Our goal is to perform a prospective study using radiofrequency ablation on sinuvertebral nerve and basivertebral nerve; evaluating its short and long term effect on pain score, disability score and patients' outcome. A review in literature is done on the pathoanatomy, pathophysiology and pain generation pathway in degenerative disc disease and chronic back pain. 30 patients with 38 levels of intervertebral disc presented with discogenic back pain with bulging degenerative intervertebral disc or spinal stenosis underwent Uniportal Full Endoscopic Radiofrequency Ablation application through either Transforaminal or Interlaminar Endoscopic Approaches. Their preoperative characteristics are recorded and prospective data was collected for Visualized Analogue Scale, Oswestry Disability Index and MacNab Criteria for pain were evaluated. There was statistically significant Visual Analogue Scale improvement from preoperative state at post-operative 1wk, 6 months and final follow up were 4.4 ± 1.0, 5.5 ± 1.2 and 5.7 ± 1.3, respectively, p < 0.0001. Oswestery Disability Index improvement from preoperative state at 1week, 6 months and final follow up were 45.8 ± 8.7, 50.4 ± 8.2 and 52.7 ± 10.3, p < 0.0001. MacNab criteria showed excellent outcomes in 17 cases, good outcomes in 11 cases and fair outcomes in 2 cases Sinuvertebral Nerve and Basivertebral Nerve Radiofrequency Ablation is effective in improving the patients' pain, disability status and patient outcome in our study.
Keywords: basivertebral nerve; degenerative disc disease; discogenic back pain; endoscopic spine surgery; lumbar spondylosis; pain management; pathophysiology of back pain; prolapsed intervertebral disc; radiofrequency ablation; sinuvertebral nerve.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures

References
-
- Vos T.P., Flaxman A.D.P., Naghavi M.P., Lozano R.P., Michaud C.M.D., Ezzati M.P., Shibuya K.P., Salomon J.A.P., Abdalla S.M., Aboyans V.P., et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2163–2196. doi: 10.1016/S0140-6736(12)61729-2. - DOI - PMC - PubMed
-
- Wong J.J., Cote P., Sutton D.A., Randhawa K., Yu H., Varatharajan S., Goldgrub R., Nordin M., Gross D.P., Shearer H.M., et al. Clinical practice guidelines for the noninvasive management of low back pain: A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur. J. Pain. 2017;21:201–216. doi: 10.1002/ejp.931. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
