

RNA-Based Strategies for Cardiac Reprogramming of Human Mesenchymal Stromal Cells
- PMID: 32098400
- PMCID: PMC7072829
- DOI: 10.3390/cells9020504
RNA-Based Strategies for Cardiac Reprogramming of Human Mesenchymal Stromal Cells
Abstract
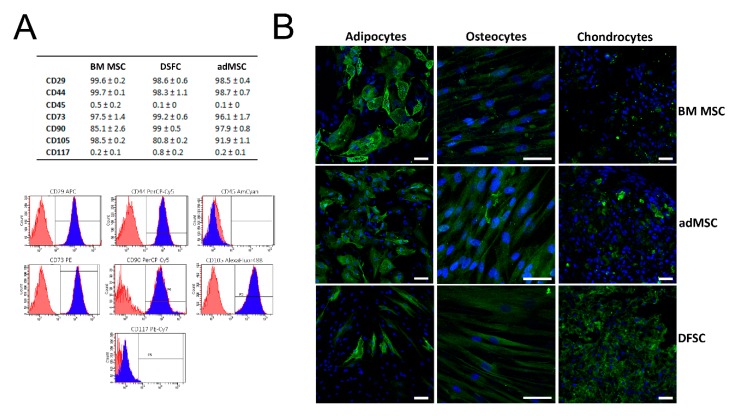
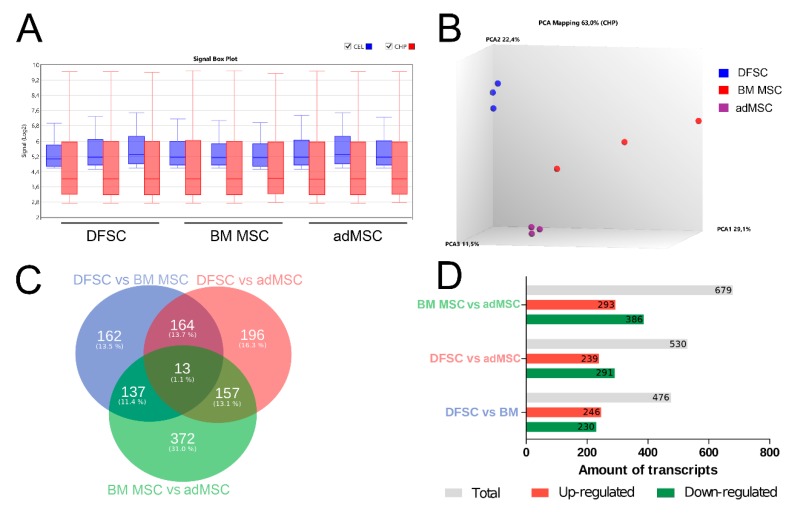
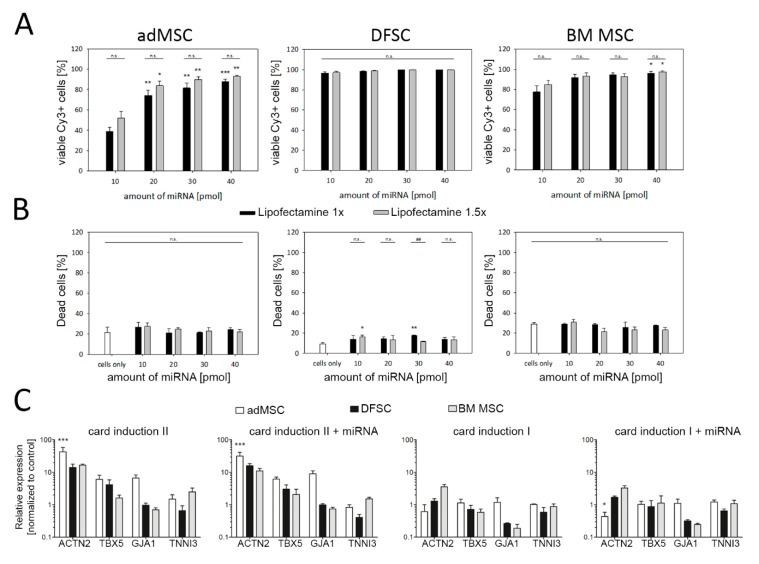
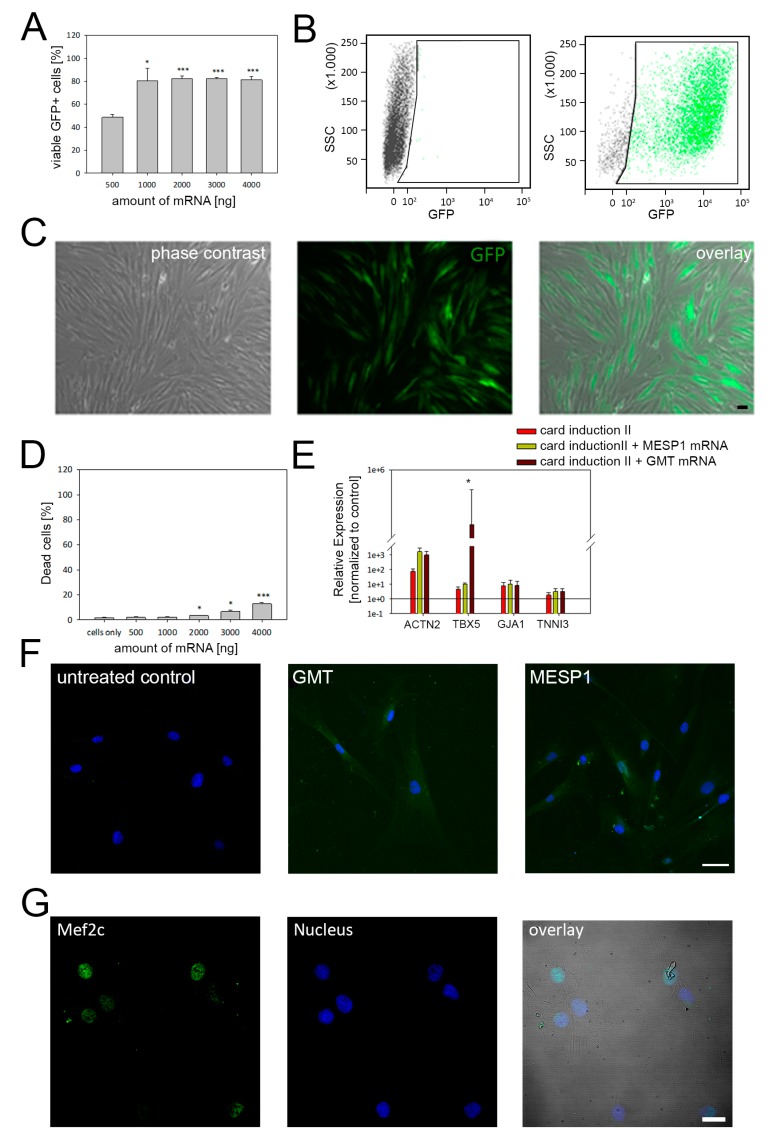
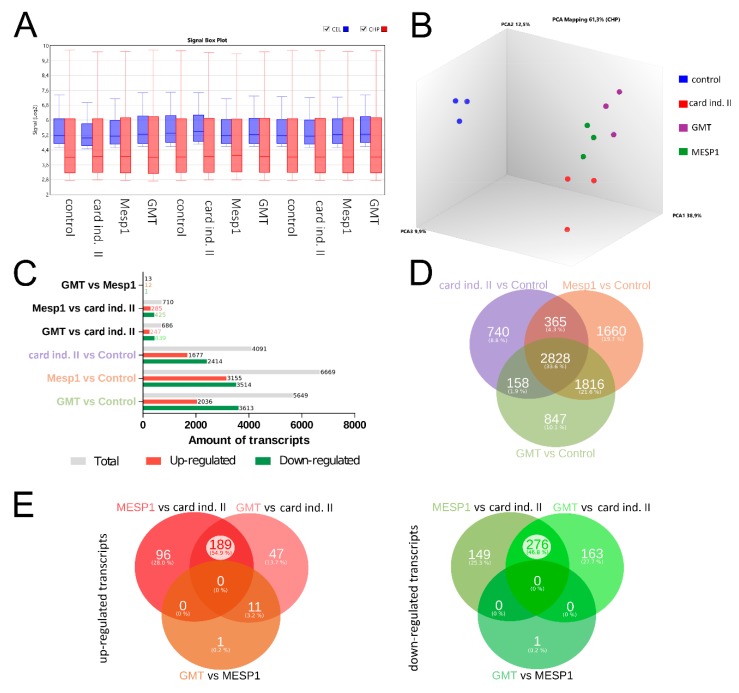
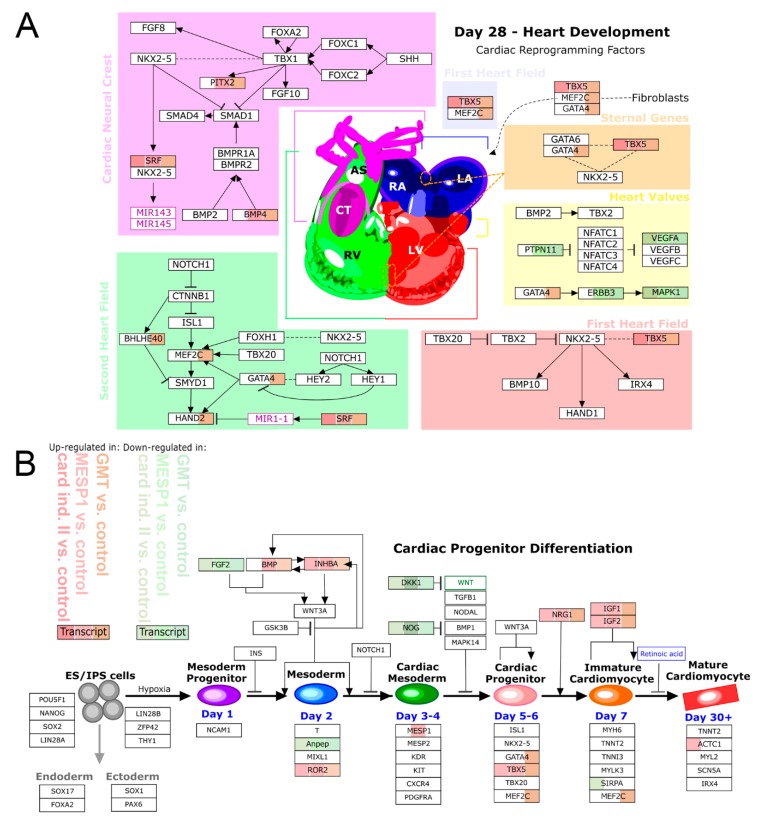
Multipotent adult mesenchymal stromal cells (MSCs) could represent an elegant source for the generation of patient-specific cardiomyocytes needed for regenerative medicine, cardiovascular research, and pharmacological studies. However, the differentiation of adult MSC into a cardiac lineage is challenging compared to embryonic stem cells or induced pluripotent stem cells. Here we used non-integrative methods, including microRNA and mRNA, for cardiac reprogramming of adult MSC derived from bone marrow, dental follicle, and adipose tissue. We found that MSC derived from adipose tissue can partly be reprogrammed into the cardiac lineage by transient overexpression of GATA4, TBX5, MEF2C, and MESP1, while cells isolated from bone marrow, and dental follicle exhibit only weak reprogramming efficiency. qRT-PCR and transcriptomic analysis revealed activation of a cardiac-specific gene program and up-regulation of genes known to promote cardiac development. Although we did not observe the formation of fully mature cardiomyocytes, our data suggests that adult MSC have the capability to acquire a cardiac-like phenotype when treated with mRNA coding for transcription factors that regulate heart development. Yet, further optimization of the reprogramming process is mandatory to increase the reprogramming efficiency.
Keywords: cardiac differentiation; cardiac reprogramming; mRNA; mesenchymal stromal cells (MSC); miRNA.
Conflict of interest statement
The authors declare no conflict of interest. The funders were not involved in study design, data collection and interpretation, and manuscript preparation.
Figures
Similar articles
-
A systemic evaluation of cardiac differentiation from mRNA reprogrammed human induced pluripotent stem cells.PLoS One. 2014 Jul 28;9(7):e103485. doi: 10.1371/journal.pone.0103485. eCollection 2014. PLoS One. 2014. PMID: 25068310 Free PMC article.
-
Human Adipose-Derived Pericytes: Biological Characterization and Reprogramming into Induced Pluripotent Stem Cells.Cell Physiol Biochem. 2020 Apr 1;54(2):271-286. doi: 10.33594/000000219. Cell Physiol Biochem. 2020. PMID: 32233339
-
The Future of Direct Cardiac Reprogramming: Any GMT Cocktail Variety?Int J Mol Sci. 2020 Oct 26;21(21):7950. doi: 10.3390/ijms21217950. Int J Mol Sci. 2020. PMID: 33114756 Free PMC article. Review.
-
Differentiation of single cell derived human mesenchymal stem cells into cells with a neuronal phenotype: RNA and microRNA expression profile.Mol Biol Rep. 2012 Apr;39(4):3995-4007. doi: 10.1007/s11033-011-1180-9. Epub 2011 Jul 20. Mol Biol Rep. 2012. PMID: 21773948
-
Genetic and Epigenetic Regulation of Human Cardiac Reprogramming and Differentiation in Regenerative Medicine.Annu Rev Genet. 2015;49:461-84. doi: 10.1146/annurev-genet-112414-054911. Annu Rev Genet. 2015. PMID: 26631515 Free PMC article. Review.
Cited by
-
Can we stop one heart from breaking: triumphs and challenges in cardiac reprogramming.Curr Opin Genet Dev. 2023 Dec;83:102116. doi: 10.1016/j.gde.2023.102116. Epub 2023 Oct 3. Curr Opin Genet Dev. 2023. PMID: 37797568 Free PMC article. Review.
-
Mesenchymal stem cell engineering by ARCA analog-capped mRNA.Mol Ther Nucleic Acids. 2023 Jul 17;33:454-468. doi: 10.1016/j.omtn.2023.07.006. eCollection 2023 Sep 12. Mol Ther Nucleic Acids. 2023. PMID: 37588684 Free PMC article.
-
Brachyury engineers cardiac repair competent stem cells.Stem Cells Transl Med. 2021 Mar;10(3):385-397. doi: 10.1002/sctm.20-0193. Epub 2020 Oct 24. Stem Cells Transl Med. 2021. PMID: 33098750 Free PMC article.
-
mRNA-Enhanced Cell Therapy and Cardiovascular Regeneration.Cells. 2021 Jan 19;10(1):187. doi: 10.3390/cells10010187. Cells. 2021. PMID: 33477787 Free PMC article. Review.
-
A preview of selected articles.Stem Cells Transl Med. 2021 Mar;10(3):333-336. doi: 10.1002/sctm.21-0036. Stem Cells Transl Med. 2021. PMID: 33619898 Free PMC article. No abstract available.
References
-
- Collichia M., Jones D.A., Beirne A.-M., Hussain M., Weeraman D., Rathod K., Veerapen J., Lowdell M., Mathur A. Umbilical cord-derived mesenchymal stromal cells in cardiovascular disease: review of preclinical and clinical data. Cytotherapy. 2019;21:1007–1018. doi: 10.1016/j.jcyt.2019.04.056. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
