

Angular deformities of lower limb in children: Correction for whom, when and how?
- PMID: 32099279
- PMCID: PMC7026560
- DOI: 10.1016/j.jcot.2020.01.008
Angular deformities of lower limb in children: Correction for whom, when and how?
Abstract
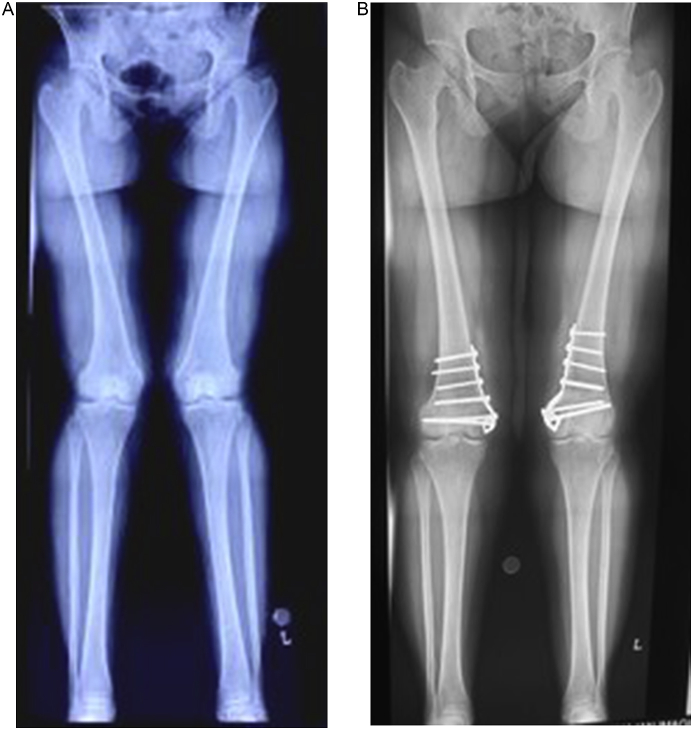
Angular deformities are common presentations in childhood and adolescent age group. It is important to differentiate a true deformity from a physiological deformity, this requires measurement of the intercondylar and intermalleolar distance. Once a true deformity is diagnosed, the apex of the deformity requires to be established. Lower limb frontal plane deformities are evaluated with a true AP standing radiographs of the entire lower limb from hip to ankle. Mechanical or anatomical axis calculation gives the apex (CORA) as well as the magnitude of deformity. Frontal plane deformities require surgical intervention. In younger children, growth modulation surgery allows correction of the deformity with minimal morbidity and without the need for osteotomy. Older children, adolescents and adults require corrective osteotomy. The corrective osteotomy can be closed wedge, open wedge, or a dome osteotomy. The osteotomy may be stabilized with internal fixation with plate and screws or an intramedullary implant as is dictated by the level of osteotomy and the local bony anatomy. External fixators allow gradual and precise correction of the deformity.
Keywords: Angular deformities; Children; Deformity correction.
© 2020 Delhi Orthopedic Association. All rights reserved.
Conflict of interest statement
The Authors declare that they have no conflict of interest with regards to the article titled.
Figures





References
-
- Akhmedov B., Ahn S., Chung C.Y. Estimation of the recovery of physiological genu varum with linear mixed model. J Pediatr Orthop. 2013;33(4):439–445. - PubMed
-
- Salenius P., Vankka E. The development of the tibiofemoral angle in children. J Bone Jt Surg Am Vol. 1975;57(2):259–261. - PubMed
-
- Yeo A., James K., Ramachandran M. Normal lower limb variants in children. BMJ. 2015;350 - PubMed
-
- Heath C.H., Staheli L.T. Normal limits of knee angle in white children--genu varum and genu valgum. J Pediatr Orthop. 1993;13(2):259–262. - PubMed
-
- O’Malley G., Hussey J., Roche E. A pilot study to profile the lower limb musculoskeletal health in children with obesity. Pediatr Phys Ther : Off Publ Sect Pediatr am Phys Ther Assoc. 2012;24(3):292–298. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
