

External Validation of an Algorithm to Identify Patients with High Data-Completeness in Electronic Health Records for Comparative Effectiveness Research
- PMID: 32099479
- PMCID: PMC7007793
- DOI: 10.2147/CLEP.S232540
External Validation of an Algorithm to Identify Patients with High Data-Completeness in Electronic Health Records for Comparative Effectiveness Research
Abstract
Objective: Electronic health records (EHR) data-discontinuity, i.e. receiving care outside of a particular EHR system, may cause misclassification of study variables. We aimed to validate an algorithm to identify patients with high EHR data-continuity to reduce such bias.
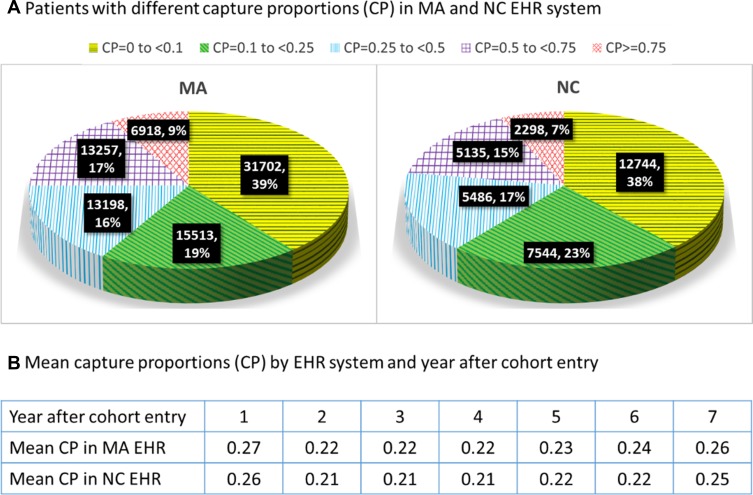
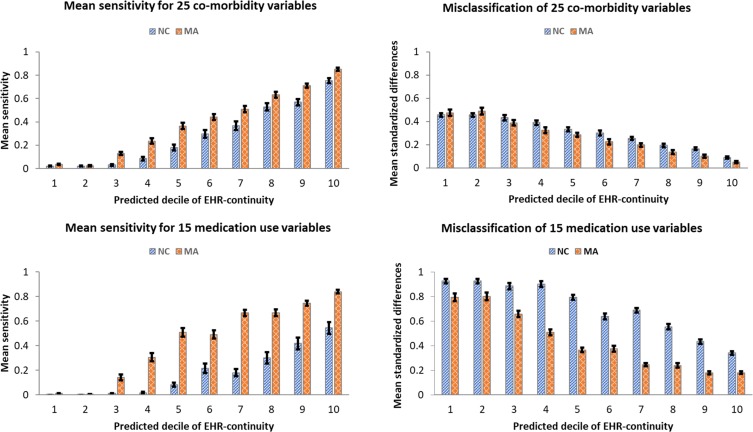
Materials and methods: We analyzed data from two EHR systems linked with Medicare claims data from 2007 through 2014, one in Massachusetts (MA, n=80,588) and the other in North Carolina (NC, n=33,207). We quantified EHR data-continuity by Mean Proportion of Encounters Captured (MPEC) by the EHR system when compared to complete recording in claims data. The prediction model for MPEC was developed in MA and validated in NC. Stratified by predicted EHR data-continuity, we quantified misclassification of 40 key variables by Mean Standardized Differences (MSD) between the proportions of these variables based on EHR alone vs the linked claims-EHR data.
Results: The mean MPEC was 27% in the MA and 26% in the NC system. The predicted and observed EHR data-continuity was highly correlated (Spearman correlation=0.78 and 0.73, respectively). The misclassification (MSD) of 40 variables in patients of the predicted EHR data-continuity cohort was significantly smaller (44%, 95% CI: 40-48%) than that in the remaining population.
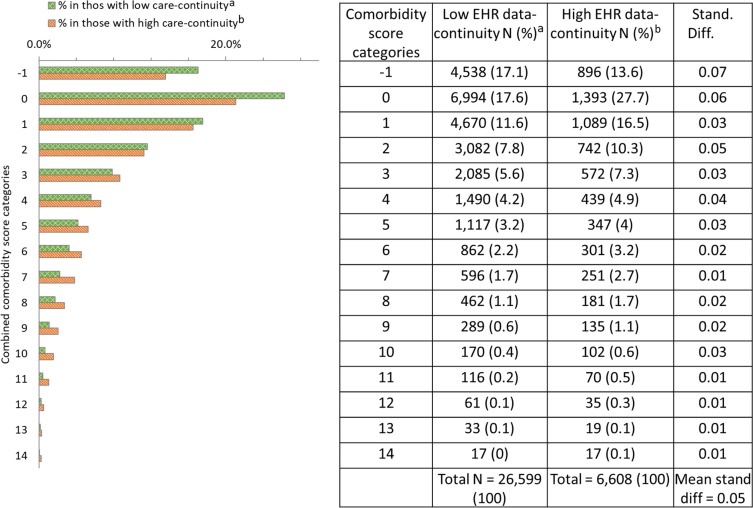
Discussion: The comorbidity profiles were similar in patients with high vs low EHR data-continuity. Therefore, restricting an analysis to patients with high EHR data-continuity may reduce information bias while preserving the representativeness of the study cohort.
Conclusion: We have successfully validated an algorithm that can identify a high EHR data-continuity cohort representative of the source population.
Keywords: comparative effectiveness research; continuity; data linkage; electronic medical records; external validation; information bias.
© 2020 Lin et al.
Conflict of interest statement
Dr Robert Glynn reports grants from Kowa, Novartis, Pfizer, and Astra Zeneca, outside the submitted work; Dr Sebastian Schneeweise reports personal fees from WHISCON, LLC, Aetion, Inc., outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
References
-
- Smith M, Stuckhardt I. Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. National Academies Press; 2012. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
