

Bone-on-Bone Anatomic Patellar Tendon Graft Anterior Cruciate Ligament Reconstruction: A Reproducible Technique Combining Press-Fit and Extracortical Fixation
- PMID: 32099773
- PMCID: PMC7029172
- DOI: 10.1016/j.eats.2019.09.024
Bone-on-Bone Anatomic Patellar Tendon Graft Anterior Cruciate Ligament Reconstruction: A Reproducible Technique Combining Press-Fit and Extracortical Fixation
Abstract
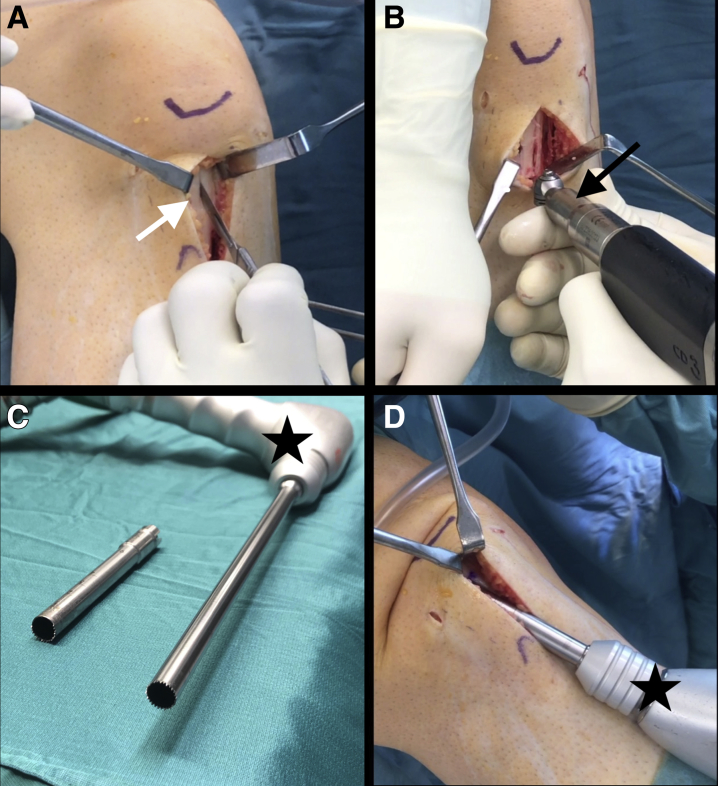
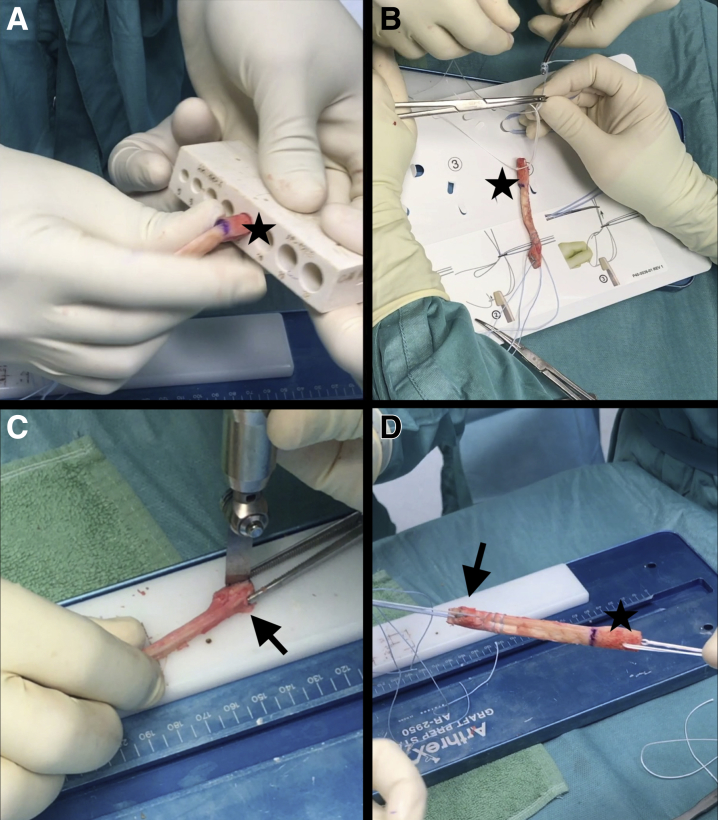
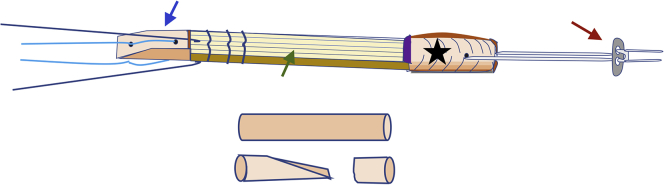
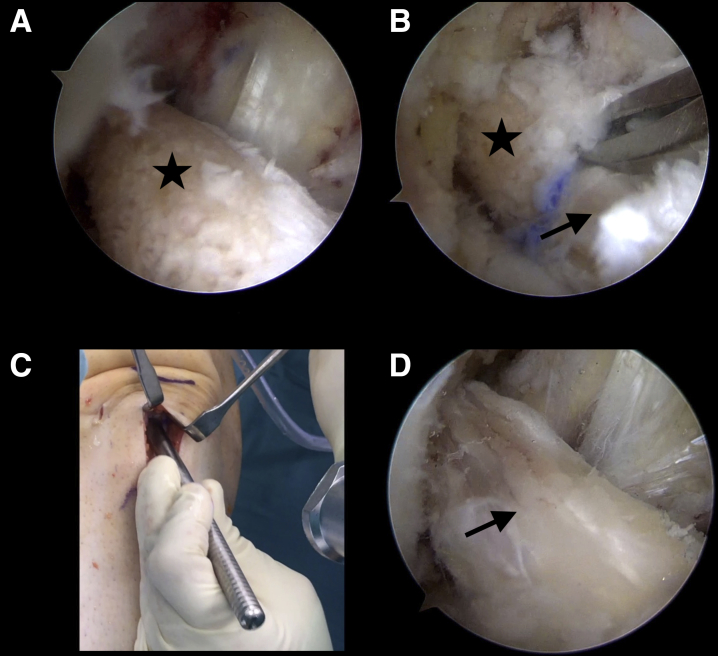
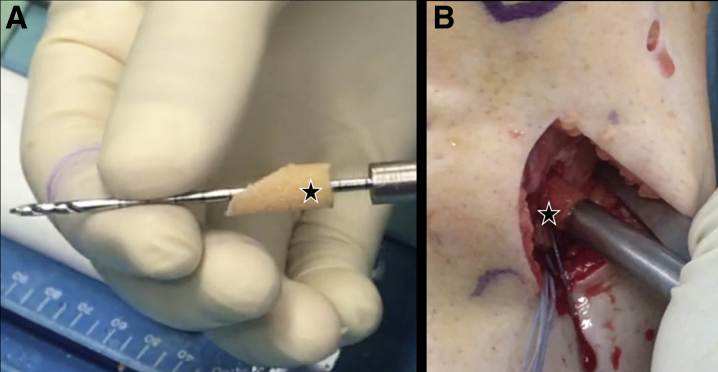
Scientific interest in optimizing outcomes after anterior cruciate ligament (ACL) reconstruction is ongoing, and some recent developments have focused on graft shape as one of the most important factors of anatomic graft placement. The double-bundle or fanlike structure of the native ACL seems to more closely restore normal function and control of rotational stability of the knee with implant-free or press-fit techniques, creating a favorable situation in terms of direct graft-tunnel healing. The ACL reconstruction technique presented in this article enables safe, reproducible, and anatomic fixation of the patellar tendon autograft, providing the biological and biomechanical benefits of direct bony integration of the ribbonlike bone-patellar tendon-bone graft. Because press-fit fixation represents a technically challenging surgical procedure, the goal of the described technique is to enable direct bone-to-bone healing by using secondary extracortical femoral and tibial fixation without the need for a true press-fit situation. Safe and anatomic femoral tunnel drilling is achieved with an outside-in technique (retrograde drilling), hence providing advantages in the routine clinical setting in terms of applicability and time effort. To reduce donor-site morbidity caused by bone block harvesting, refilling of the harvest sites with autologous material is performed.
© 2019 by the Arthroscopy Association of North America. Published by Elsevier.
Figures

References
-
- Wipfler B., Donner S., Zechmann C.M., Springer J., Siebold R., Paessler H.H. Anterior cruciate ligament reconstruction using patellar tendon versus hamstring tendon: A prospective comparative study with 9-year follow-up. Arthroscopy. 2011;27:653–665. - PubMed
-
- Sheean A.J., Musahl V., Slone H.S. Quadriceps tendon autograft for arthroscopic knee ligament reconstruction: Use it now, use it often. Br J Sports Med. 2018;52:698–701. - PubMed
-
- Gifstad T., Foss O.A., Engebretsen L. Lower risk of revision with patellar tendon autografts compared with hamstring autografts: A registry study based on 45,998 primary ACL reconstructions in Scandinavia. Am J Sports Med. 2014;42:2319–2328. - PubMed
-
- Boszotta H. Arthroscopic anterior cruciate ligament reconstruction using a patellar tendon graft in press-fit technique: Surgical technique and follow-up. Arthroscopy. 1997;13:332–339. - PubMed
-
- Robin B.N., Jani S.S., Marvil S.C., Reid J.B., Schillhammer C.K., Lubowitz J.H. Advantages and disadvantages of transtibial, anteromedial portal, and outside-in femoral tunnel drilling in single-bundle anterior cruciate ligament reconstruction: A systematic review. Arthroscopy. 2015;31:1412–1417. - PubMed
LinkOut - more resources
Full Text Sources
