

Anterior Cruciate Ligament Reconstruction Using a Ribbon-Like Graft With a C-Shaped Tibial Bone Tunnel
- PMID: 32099779
- PMCID: PMC7029192
- DOI: 10.1016/j.eats.2019.10.005
Anterior Cruciate Ligament Reconstruction Using a Ribbon-Like Graft With a C-Shaped Tibial Bone Tunnel
Abstract
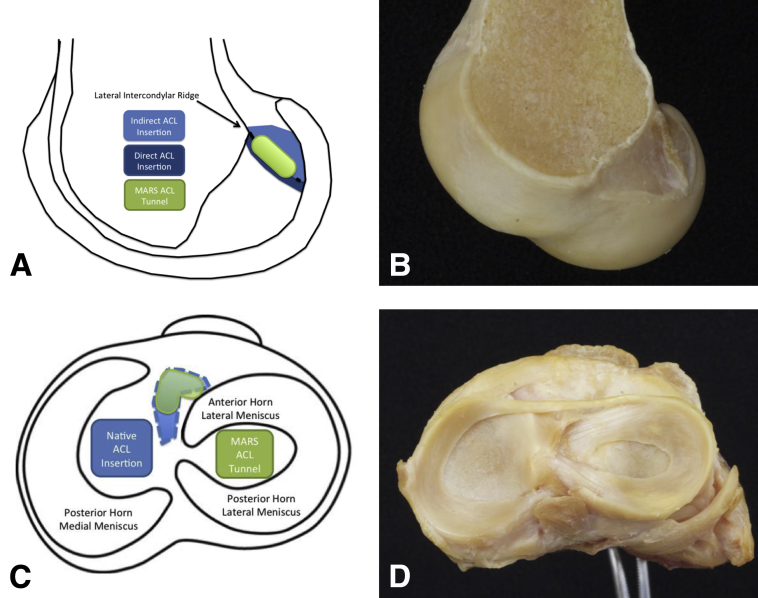
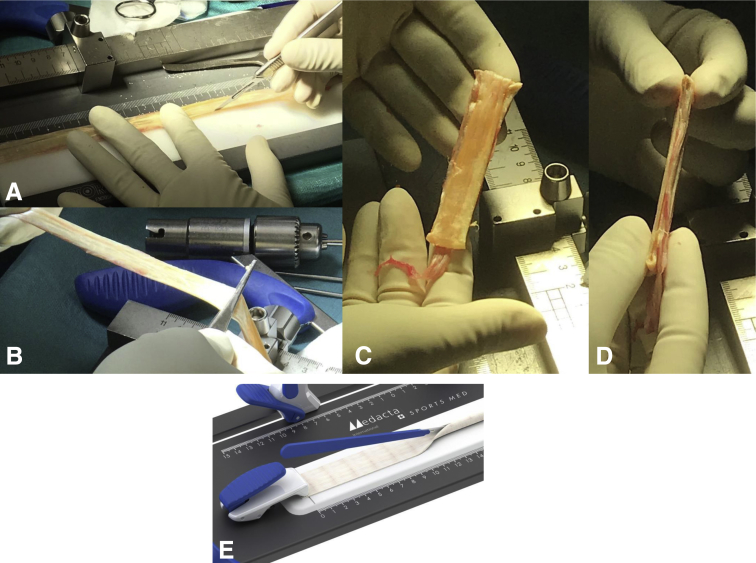
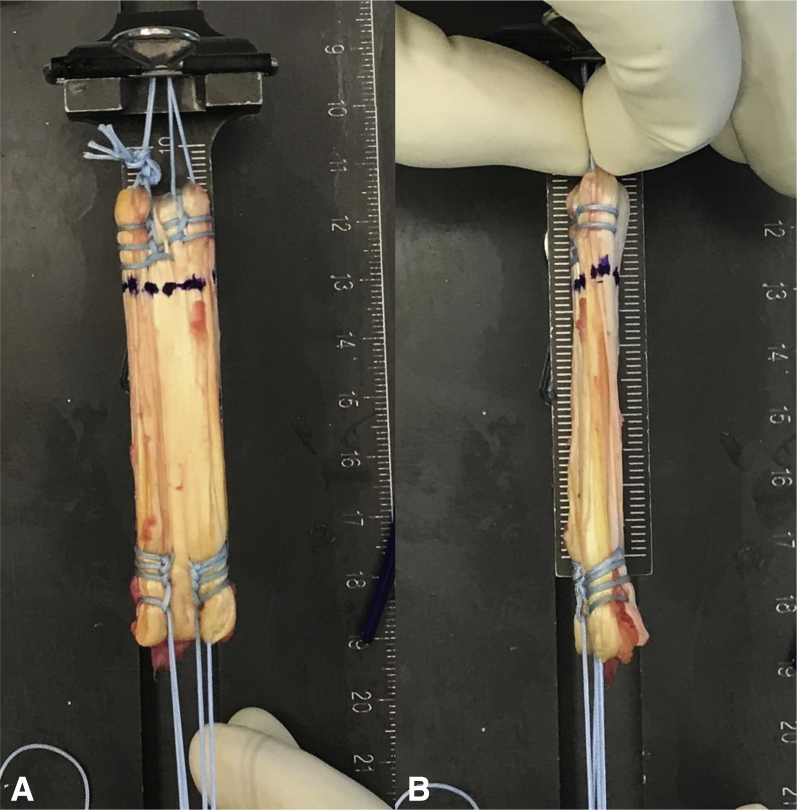
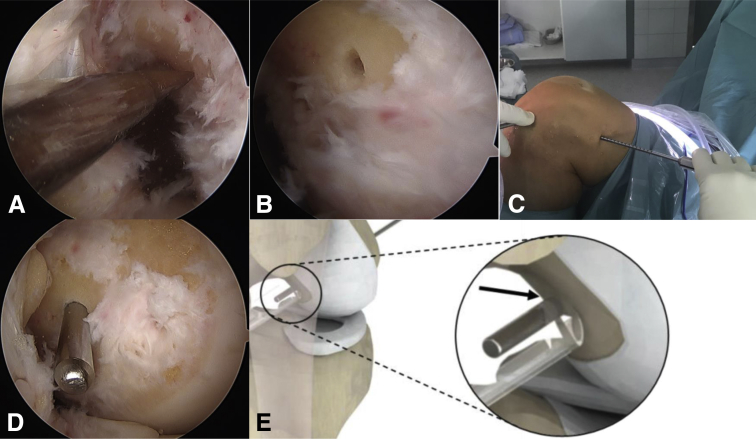
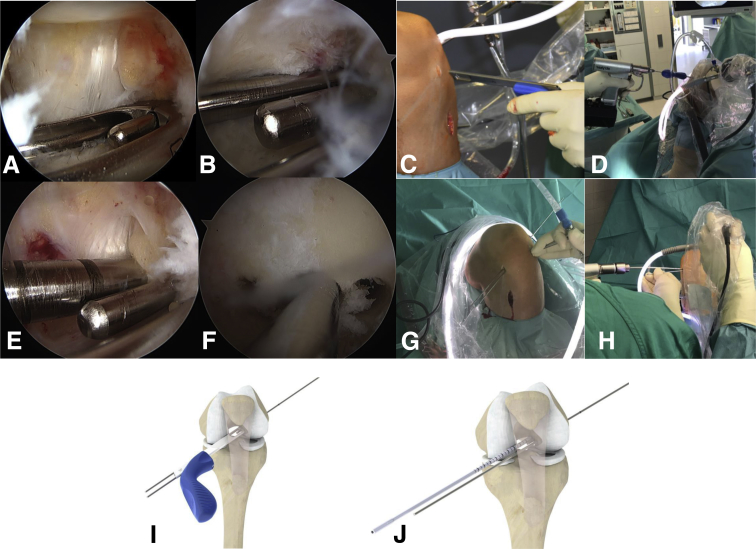
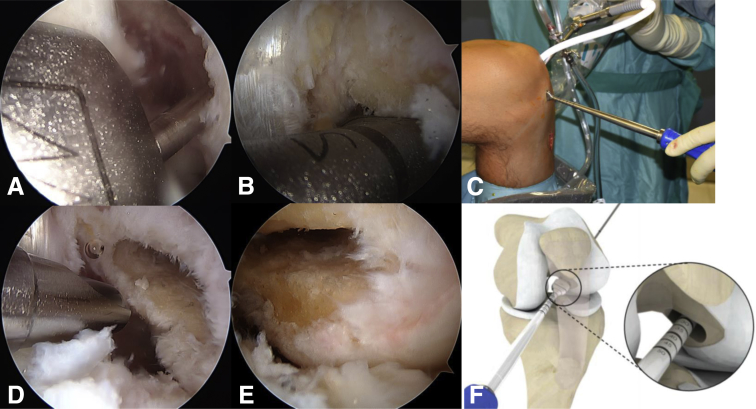
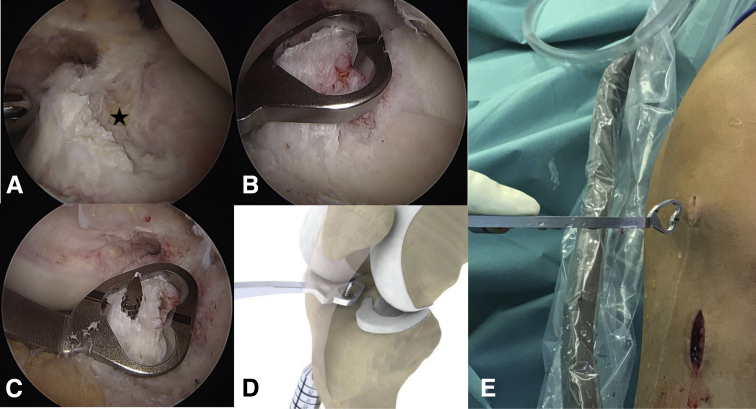
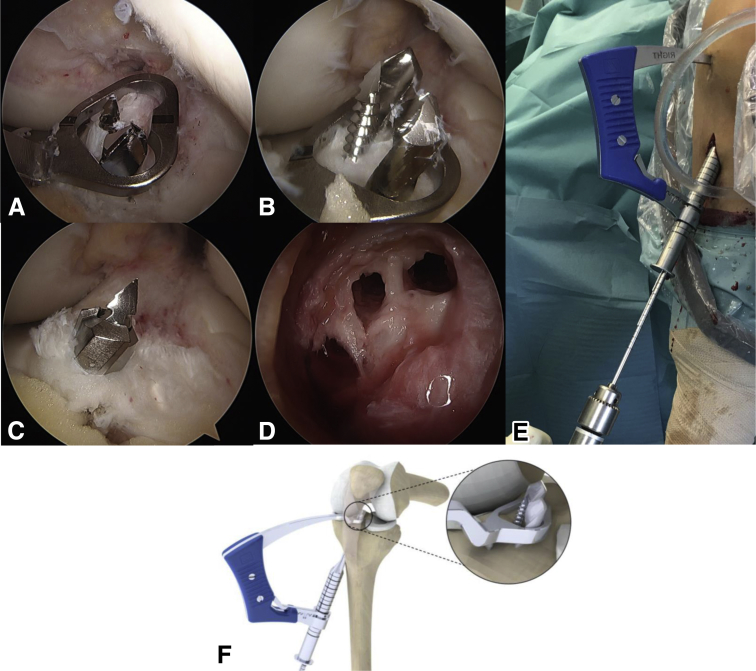
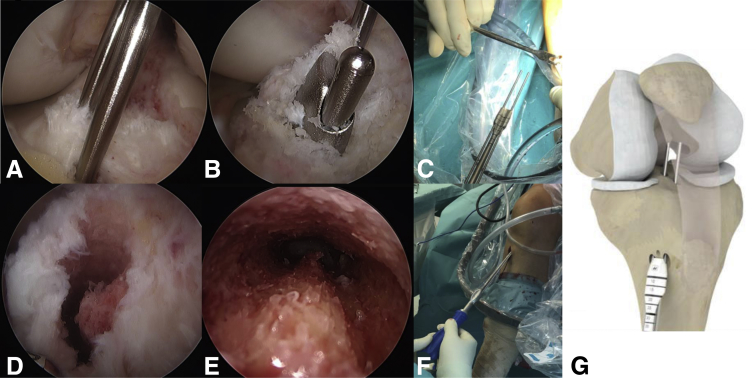
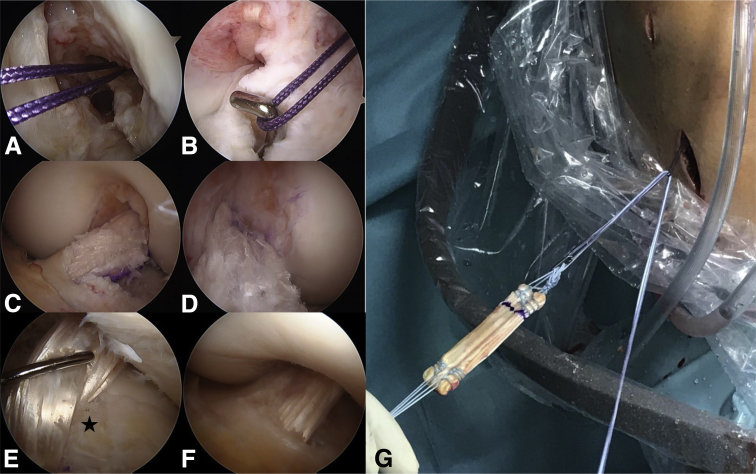
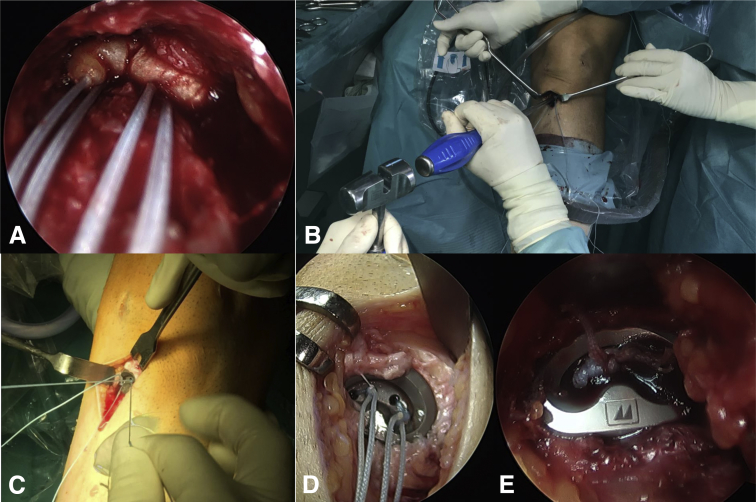
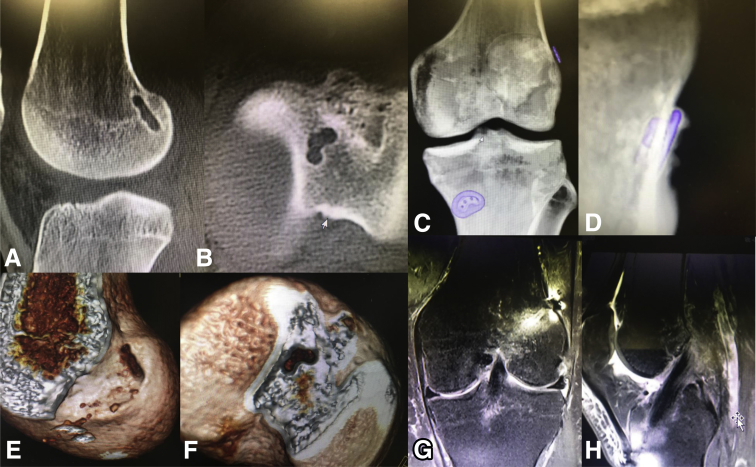
According to recent anatomic studies, the anterior cruciate ligament (ACL) appears to be a flat, "ribbon-like" structure, with a thin, oval-shaped insertion on the femur and a C-shaped tibial insertion. According to this anatomy, we describe an ACL-reconstruction technique that aims to approximate this natural anatomy. The basic principle of this technique is not to use conventional round tunnels but create tunnel shapes that resemble more closely the original ACL insertion sites. Using either a rectangular quadriceps tendon graft or a "flat" hamstring graft may not only provide a biomechanical advantage with increased rotational stability but also improve bone-tendon healing due to increased bone-tendon contact and decreased diffusion length. Creating a C-shaped tibial tunnel also avoids laceration of the anterior horn of the lateral meniscus, which is frequently harmed during conventional tibial tunnel drilling.
© 2019 by the Arthroscopy Association of North America. Published by Elsevier.
Figures
References
-
- Mochizuki T., Muneta T., Nagase T., Shirasawa S., Akita K.I., Sekiya I. Cadaveric knee observation study for describing anatomic femoral tunnel placement for two-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2006;22:356–361. - PubMed
-
- Kyung B.S., Kim J.G., Chang M., Jang K.M., Lee S.S., Ahn J.H. Anatomic double-bundle reconstruction techniques result in graft obliquities that closely mimic the native anterior cruciate ligament anatomy. Am J Sports Med. 2013;41:1302–1309. - PubMed
-
- Smigielski R., Zdanowicz U., Drwiega M., Ciszek B., Williams A. The anatomy of the anterior cruciate ligament and its relevance to the technique of reconstruction. Bone Joint J. 2016;98-B:1020–1026. - PubMed
-
- Smigielski R., Zdanowicz U., Drwiega M., Ciszek B., Ciszkowska-Lyson B., Siebold R. Ribbon like appearance of the midsubstance fibres of the anterior cruciate ligament close to its femoral insertion site: A cadaveric study including 111 knees. Knee Surg Sports Traumatol Arthrosc. 2015;23:3143–3150. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
