

Maternal Prenatal Psychosocial Stress and Prepregnancy BMI Associations with Fetal Iron Status
- PMID: 32099952
- PMCID: PMC7026381
- DOI: 10.1093/cdn/nzaa018
Maternal Prenatal Psychosocial Stress and Prepregnancy BMI Associations with Fetal Iron Status
Abstract
Background: Iron accrued in utero is critical for fetal and infant neurocognitive development. Psychosocial stress and obesity can each suppress fetal iron accrual. Their combined effects and differences by fetal sex are not known. In an observational pregnancy cohort study in Mexico City, we investigated associations of maternal prenatal life stressors, psychological dysfunction, and prepregnancy BMI with fetal iron status at delivery.
Objectives: We hypothesized that greater maternal prenatal psychosocial stress and prepregnancy overweight and obesity are associated with lower cord blood ferritin and hemoglobin (Hb), with stronger associations in boys than girls.
Methods: Psychosocial stress in multiple domains of life stress (negative life events, perceived stress, exposure to violence) and psychological dysfunction symptoms (depression, generalized anxiety, and pregnancy-specific anxiety) were assessed with validated questionnaires during pregnancy. Prepregnancy BMI was predicted with a validated equation and categorized as normal/overweight/obese. Cord blood ferritin and Hb associations with prenatal psychosocial stress and BMI were modeled in multivariable linear regressions adjusted for maternal age, socioeconomic status, child sex, and prenatal iron supplementation. Interactions with child sex and 3-way stress-overweight/obesity-sex interactions were tested with product terms and likelihood ratio tests.
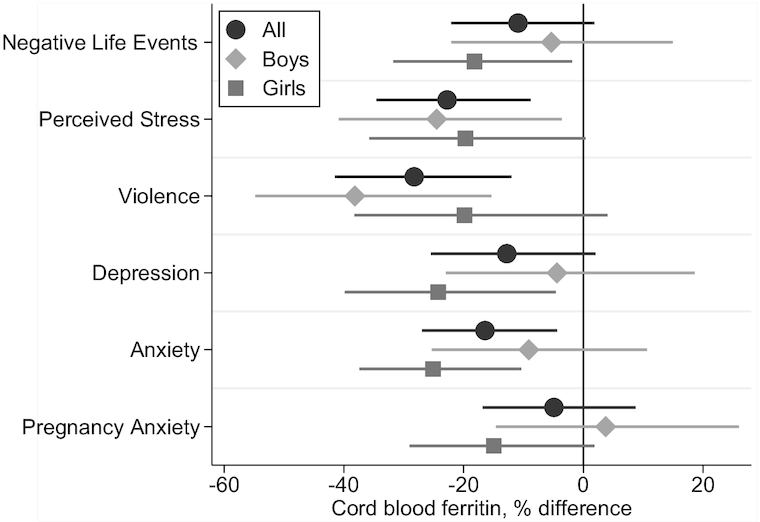
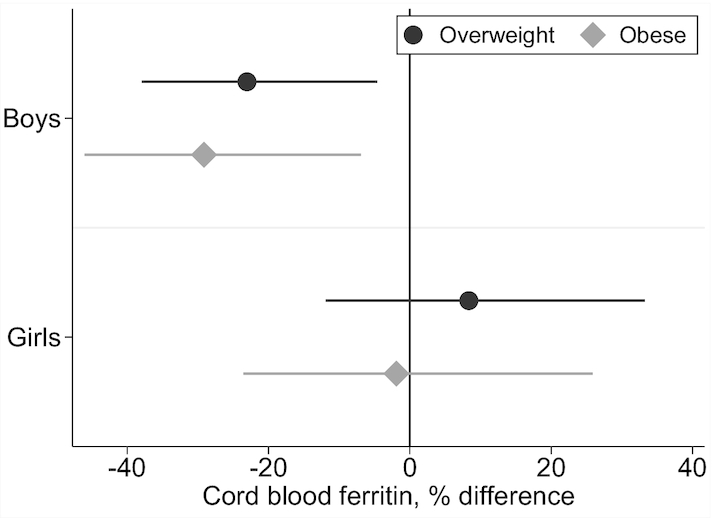
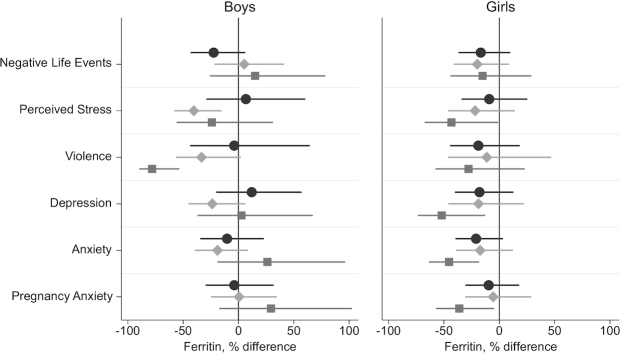
Results: In 493 dyads, median (IQR) cord blood ferritin and Hb concentrations were 185 µg/L (126-263 g/dL) and 16 g/dL (14.7-17.1 g/dL), respectively. Ferritin was lower in infants of mothers with higher prenatal perceived stress (-23%; 95% CI: -35%, -9%), violence exposure (-28%; 95% CI: -42%, -12%), anxiety symptoms (-16%; 95% CI: -27%, -4%), and obesity (-17%; 95% CI: -31%, 0.2%). Interaction models suggested sex differences and synergism between maternal stress and overweight/obesity. No associations were observed between stress or BMI and Hb.
Conclusions: Multiple prenatal psychosocial stressors and excess prepregnancy BMI were each inversely associated with fetal iron status at birth. Pregnancies and infants at elevated risk of impaired fetal iron accrual may be identifiable according to observed synergism between maternal stress and obesity and differential associations with fetal iron status by infant sex.
Keywords: Mexico; anxiety; depression; developmental origins of health and disease (DOHAD); exposure to violence; iron deficiency; maternal health; negative life events; pregnancy.
Copyright © The Author(s) 2020.
Figures
References
-
- Black MM, Quigg AM, Hurley KM, Pepper MR. Iron deficiency and iron-deficiency anemia in the first two years of life: strategies to prevent loss of developmental potential. Nutr Rev. 2011;69(Suppl 1):S64–70. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
