

Changing care pathways and between-center practice variations in intensive care for traumatic brain injury across Europe: a CENTER-TBI analysis
- PMID: 32100061
- PMCID: PMC7210239
- DOI: 10.1007/s00134-020-05965-z
Changing care pathways and between-center practice variations in intensive care for traumatic brain injury across Europe: a CENTER-TBI analysis
Abstract
Purpose: To describe ICU stay, selected management aspects, and outcome of Intensive Care Unit (ICU) patients with traumatic brain injury (TBI) in Europe, and to quantify variation across centers.
Methods: This is a prospective observational multicenter study conducted across 18 countries in Europe and Israel. Admission characteristics, clinical data, and outcome were described at patient- and center levels. Between-center variation in the total ICU population was quantified with the median odds ratio (MOR), with correction for case-mix and random variation between centers.
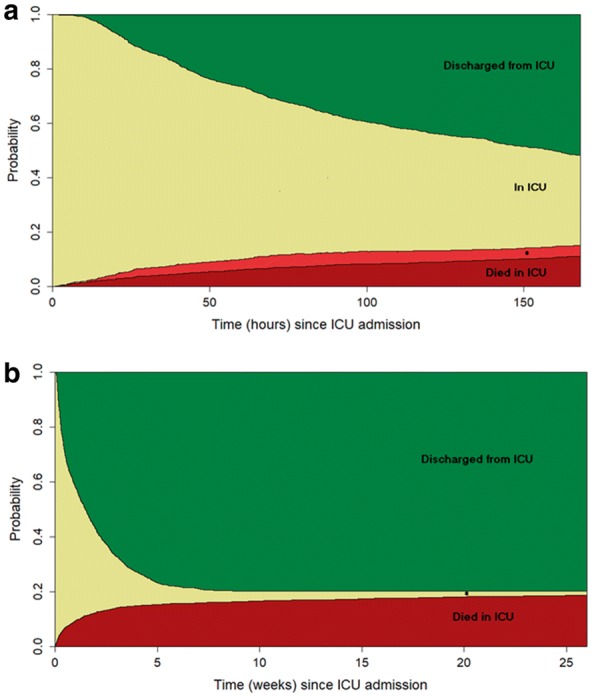
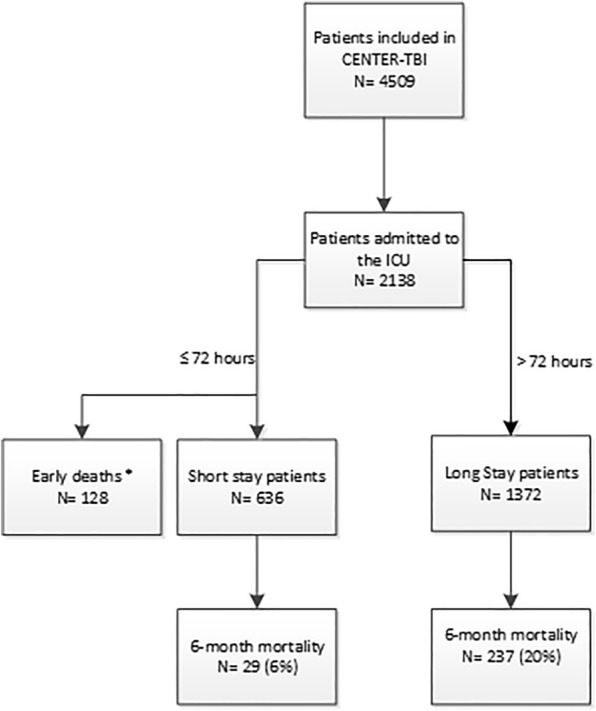
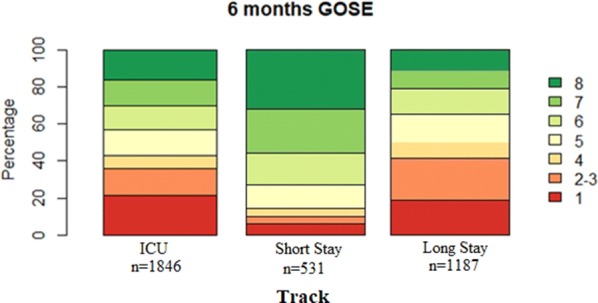
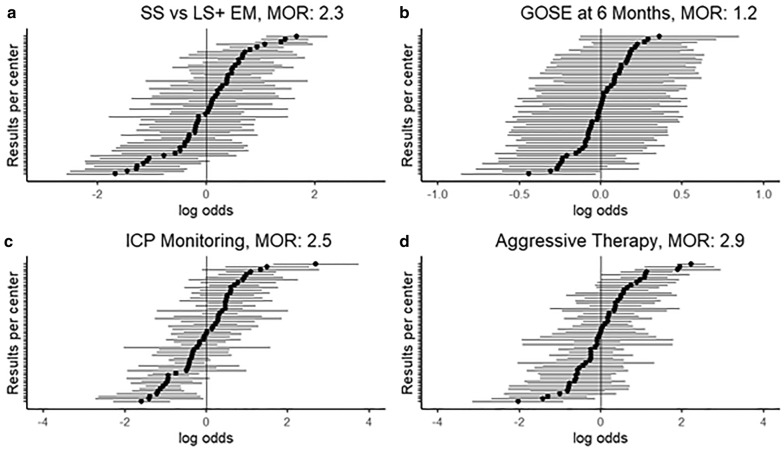
Results: A total of 2138 patients were admitted to the ICU, with median age of 49 years; 36% of which were mild TBI (Glasgow Coma Scale; GCS 13-15). Within, 72 h 636 (30%) were discharged and 128 (6%) died. Early deaths and long-stay patients (> 72 h) had more severe injuries based on the GCS and neuroimaging characteristics, compared with short-stay patients. Long-stay patients received more monitoring and were treated at higher intensity, and experienced worse 6-month outcome compared to short-stay patients. Between-center variations were prominent in the proportion of short-stay patients (MOR = 2.3, p < 0.001), use of intracranial pressure (ICP) monitoring (MOR = 2.5, p < 0.001) and aggressive treatments (MOR = 2.9, p < 0.001); and smaller in 6-month outcome (MOR = 1.2, p = 0.01).
Conclusions: Half of contemporary TBI patients at the ICU have mild to moderate head injury. Substantial between-center variations exist in ICU stay and treatment policies, and less so in outcome. It remains unclear whether admission of short-stay patients represents appropriate prudence or inappropriate use of clinical resources.
Keywords: Intensive care unit; Intracranial pressure; Outcome; Traumatic brain injury.
Conflict of interest statement
AIRM declares consulting fees from PresSura Neuro, Integra Life Sciences, and NeuroTrauma Sciences. DKM reports grants from the UK National Institute for Health Research, during the conduct of the study; grants, personal fees, and non-financial support from GlaxoSmithKline; personal fees from Neurotrauma Sciences, Lantmaanen AB, Pressura, and Pfizer, outside of the submitted work. WP reports grants from the Netherlands Brain Foundation. ES reports personal fees from Springer, during the conduct of the study. All other authors declare no competing interests.
Figures
References
-
- Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, Napolitano LM, O’Grady NP, Bartlett JG, Carratala J, El Solh AA, Ewig S, Fey PD, File TM, Jr, Restrepo MI, Roberts JA, Waterer GW, Cruse P, Knight SL, Brozek JL. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63:e61–e111. doi: 10.1093/cid/ciw353. - DOI - PMC - PubMed
-
- Steyerberg EW, Wiegers E, Sewalt C, Buki A, Citerio G, De Keyser V, Ercole A, Kunzmann K, Lanyon L, Lecky F, Lingsma H, Manley G, Nelson D, Peul W, Stocchetti N, von Steinbuchel N, Vande Vyvere T, Verheyden J, Wilson L, Maas AIR, Menon DK, Participants C-T, Investigators Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: a European prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019;18:923–934. doi: 10.1016/S1474-4422(19)30232-7. - DOI - PubMed
-
- Volovici V, Ercole A, Citerio G, Stocchetti N, Haitsma IK, Huijben JA, Dirven CMF, van der Jagt M, Steyerberg EW, Nelson D, Cnossen MC, Maas AIR, Polinder S, Menon DK, Lingsma HF. Intensive care admission criteria for traumatic brain injury patients across Europe. J Crit Care. 2019;49:158–161. doi: 10.1016/j.jcrc.2018.11.002. - DOI - PubMed
