

Gaps in the Management of Depression Symptoms Following Cancer Diagnosis: A Population-Based Analysis of Prospective Patient-Reported Outcomes
- PMID: 32100906
- PMCID: PMC7356756
- DOI: 10.1634/theoncologist.2019-0709
Gaps in the Management of Depression Symptoms Following Cancer Diagnosis: A Population-Based Analysis of Prospective Patient-Reported Outcomes
Abstract
Background: One of the most common psychological morbidities of cancer is depression. Routine depression symptoms screening (DSS) is recommended, but its ability to lead to psychosocial interventions in clinical practice is limited. We examined the use of and factors associated with psychosocial interventions for positive DSS following cancer diagnosis.
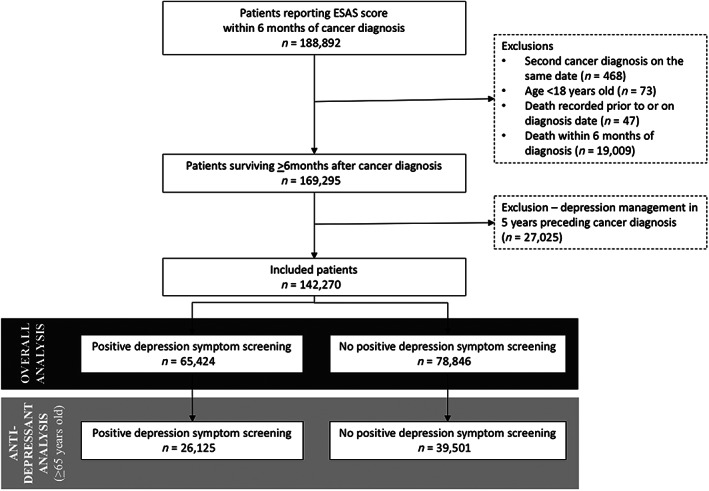
Materials and methods: We conducted a population-based cohort study of patients with diagnoses from 2010 to 2017 who reported ≥1 patient-reported Edmonton Symptom Assessment System (ESAS) score. Positive DSS was defined as ESAS ≥2 out of 10 for the depression item within 6 months of diagnosis. Outcomes were psychosocial interventions around the time of positive DSS: palliative care assessment, psychiatry/psychology assessment, social work referral, and antidepressant therapy (in patients ≥65 years of age with universal drug coverage). We examined reduction in depression symptom score (≥1 point) following intervention. Modified Poisson regression examined factors associated with interventions.
Results: Of 142,270 patients, 65,424 (46.0%) reported positive DSS at a median of 66 days (interquartile range: 34-105) after diagnosis. Of those with depression symptoms, 17.1% received palliative assessment, 1.7% psychiatry/psychology assessment, 8.4% social work referral, and 4.3% antidepressant therapy. Depression symptom score decreased in 67.2% who received palliative assessment, 63.7% with psychiatry/psychology assessment, 67.3% with social work referral, and 71.4% with antidepressant therapy. On multivariable analysis, patients with older age, rural residence, lowest income quintile, and genitourinary or oropharyngeal cancer were more likely to not receive intervention other than palliative care.
Conclusion: The proportion of patients reporting positive DSS after cancer diagnosis receiving psychosocial intervention is low. We identified patients vulnerable to not receiving interventions, who may benefit from additional support. These data represent a call to action to modify practice and optimize the usefulness of systematic symptom screening.
Implications for practice: Patient-reported depression symptoms screening should be followed by targeted interventions to improve symptoms and patient-centered management.
Keywords: Depression; Distress; Patient-reported outcomes; Supportive care.
© AlphaMed Press 2020.
Conflict of interest statement
Figures



Similar articles
-
A population-based analysis of the management of symptoms of depression among patients with stage IV non-small cell lung cancer (NSCLC) in Ontario, Canada.Support Care Cancer. 2024 May 24;32(6):381. doi: 10.1007/s00520-024-08584-2. Support Care Cancer. 2024. PMID: 38787434
-
Gaps in Depression Symptom Management for Patients With Head and Neck Cancer.Laryngoscope. 2023 Oct;133(10):2638-2646. doi: 10.1002/lary.30595. Epub 2023 Feb 7. Laryngoscope. 2023. PMID: 36748910
-
The impact of routine Edmonton symptom assessment system use on receiving palliative care services: results of a population-based retrospective-matched cohort analysis.BMJ Support Palliat Care. 2023 Oct;13(e1):e144-e149. doi: 10.1136/bmjspcare-2020-002220. Epub 2020 Sep 17. BMJ Support Palliat Care. 2023. PMID: 32943469
-
Telephone interventions for symptom management in adults with cancer.Cochrane Database Syst Rev. 2020 Jun 2;6(6):CD007568. doi: 10.1002/14651858.CD007568.pub2. Cochrane Database Syst Rev. 2020. PMID: 32483832 Free PMC article.
-
National Institutes of Health State-of-the-Science Conference Statement: Symptom management in cancer: pain, depression, and fatigue, July 15-17, 2002.J Natl Cancer Inst Monogr. 2004;(32):9-16. doi: 10.1093/jncimonographs/djg014. J Natl Cancer Inst Monogr. 2004. PMID: 15263035 Review.
Cited by
-
Depression, Anxiety, and Patterns of Mental Health Care Among Men With Prostate Cancer Receiving Androgen Deprivation Therapy.Oncologist. 2022 Apr 5;27(4):314-322. doi: 10.1093/oncolo/oyab033. Oncologist. 2022. PMID: 35298660 Free PMC article.
-
Demoralization level fluctuated at various time frame of radiotherapy for patients with different cancers: a longitudinal observational study.BMC Palliat Care. 2022 Aug 10;21(1):143. doi: 10.1186/s12904-022-01033-z. BMC Palliat Care. 2022. PMID: 35948925 Free PMC article.
-
Symptom burden in transplant ineligible patients with newly diagnosed multiple myeloma: a population-based cohort study.Haematologica. 2021 Jul 1;106(7):1991-1994. doi: 10.3324/haematol.2020.267757. Haematologica. 2021. PMID: 33353286 Free PMC article.
-
Incidence of and Factors Associated With Nonfatal Self-injury After a Cancer Diagnosis in Ontario, Canada.JAMA Netw Open. 2021 Sep 1;4(9):e2126822. doi: 10.1001/jamanetworkopen.2021.26822. JAMA Netw Open. 2021. PMID: 34559226 Free PMC article.
-
Enhancing Outpatient Symptom Management in Patients With Head and Neck Cancer: A Qualitative Analysis.JAMA Otolaryngol Head Neck Surg. 2022 Apr 1;148(4):333-341. doi: 10.1001/jamaoto.2021.4555. JAMA Otolaryngol Head Neck Surg. 2022. PMID: 35238872 Free PMC article.
References
-
- Mitchell AJ, Chan M, Bhatti H et al. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative‐care settings: A meta‐analysis of 94 interview‐based studies. Lancet Oncol 2011;12:160–174. - PubMed
-
- Mojtabai R, Jorm AF. Trends in psychological distress, depressive episodes and mental health treatment‐seeking in the United States: 2001‐2012. J Affect Disord 2015;174:556–561. - PubMed
-
- Holland JC, Bultz BD, National Comprehensive Cancer Network (NCCN) . The NCCN guideline for distress management: A case for making distress the sixth vital sign. J Natl Compr Canc Netw 2007;5:3–7. - PubMed
-
- Bultz BD, Groff SL, Fitch M et al. Implementing screening for distress, the 6th vital sign: A Canadian strategy for changing practice. Psychooncology 2011;20:463–469. - PubMed
-
- DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: Meta‐analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med 2000;160:2101–2107. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
