

Lack of discreet colocalization of epithelial apoptosis to the atretic precursor in the colon of the Fibroblast growth factor receptor 2IIIb mouse and staining consistent with cellular movement suggest a revised model of atresia formation
- PMID: 32100913
- PMCID: PMC7266729
- DOI: 10.1002/dvdy.164
Lack of discreet colocalization of epithelial apoptosis to the atretic precursor in the colon of the Fibroblast growth factor receptor 2IIIb mouse and staining consistent with cellular movement suggest a revised model of atresia formation
Abstract
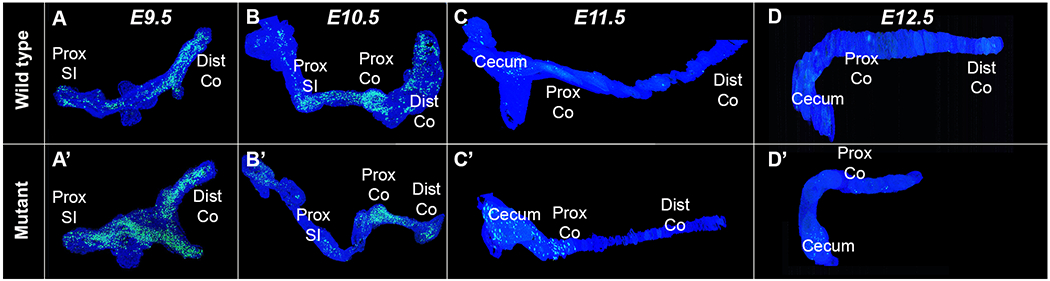
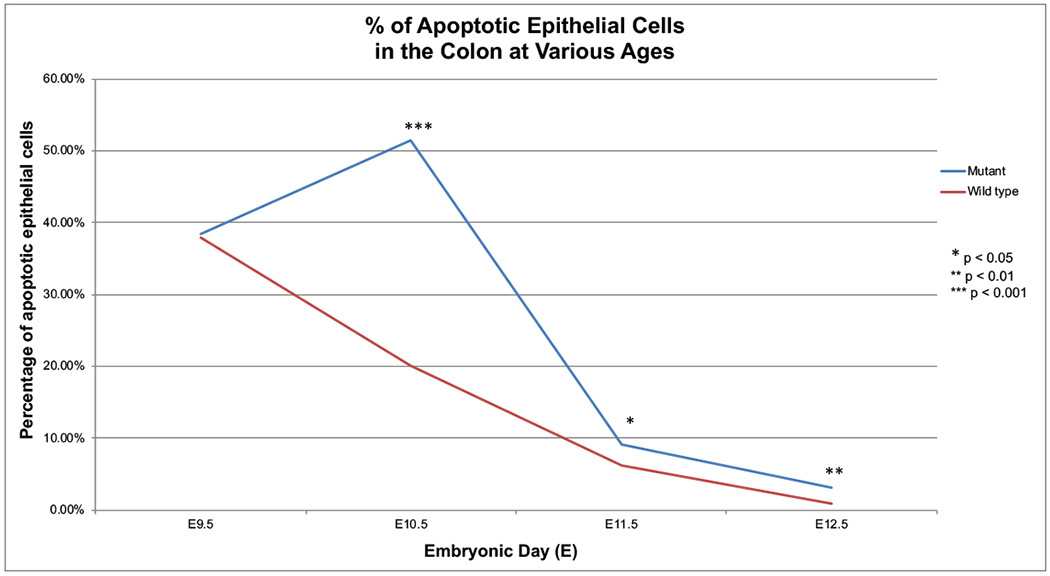
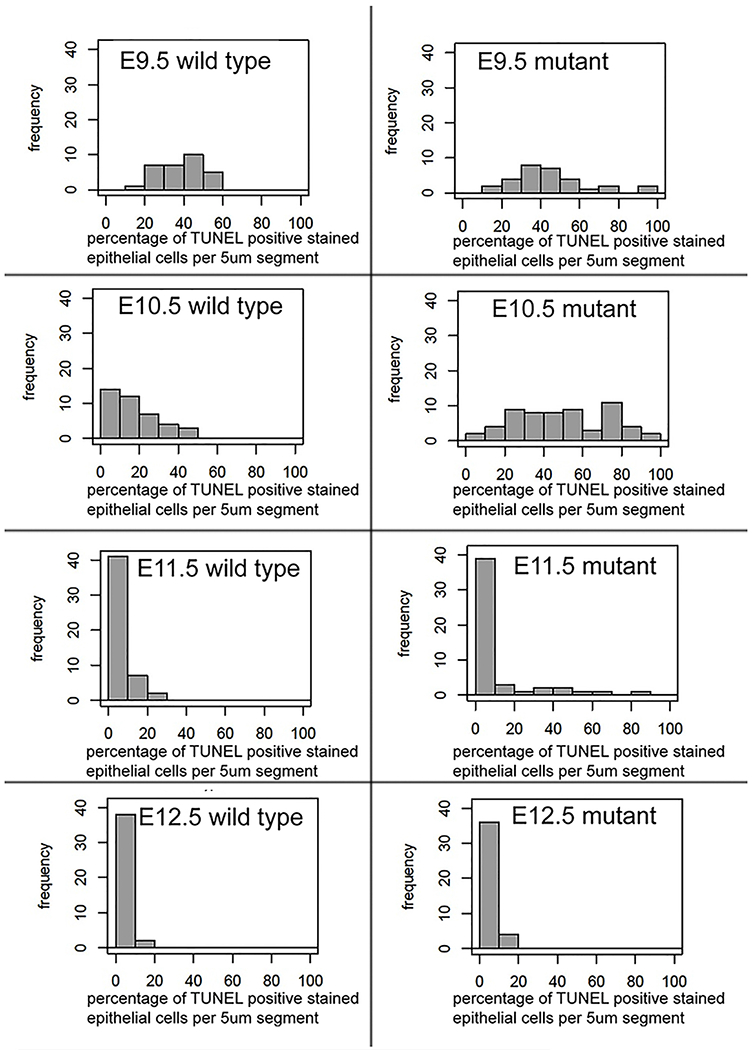
Background: Colonic atresias in the Fibroblast growth factor receptor 2IIIb (Fgfr2IIIb) mouse model have been attributed to increased epithelial apoptosis and decreased epithelial proliferation at embryonic day (E) 10.5. We therefore hypothesized that these processes would colocalize to the distal colon where atresias occur (atretic precursor) and would be excluded or minimized from the proximal colon and small intestine.
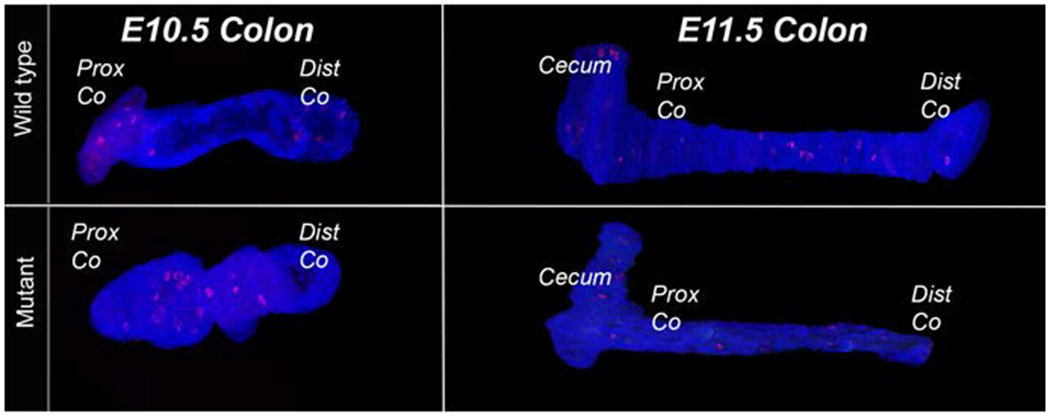
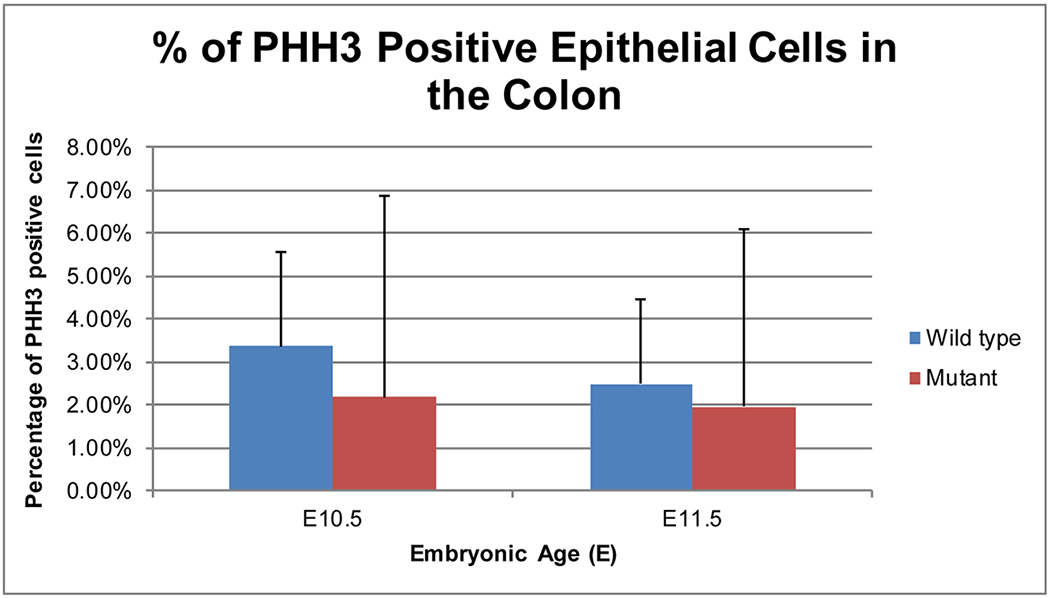
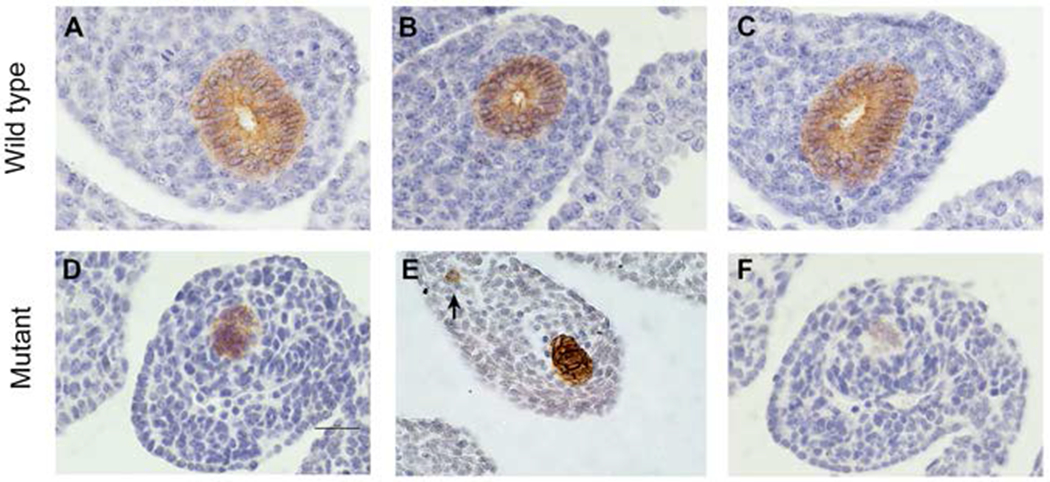
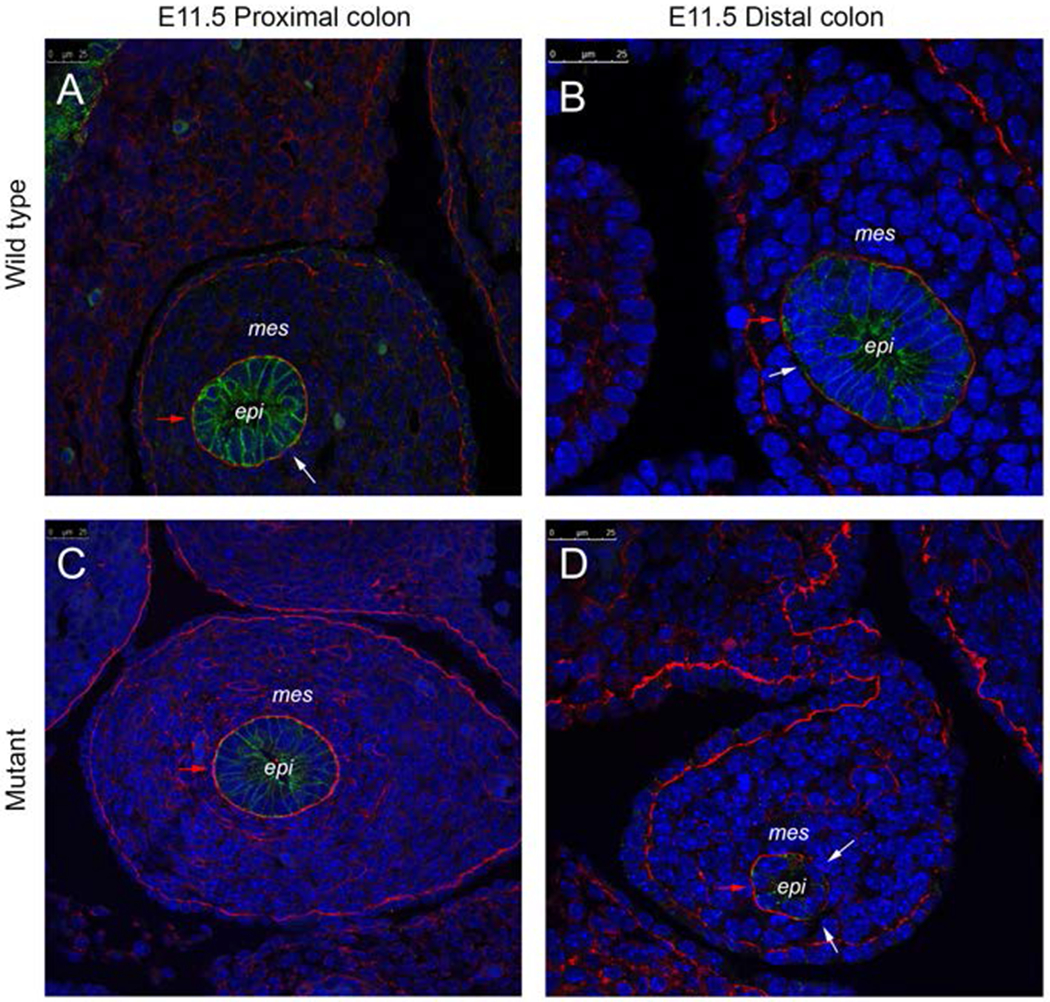
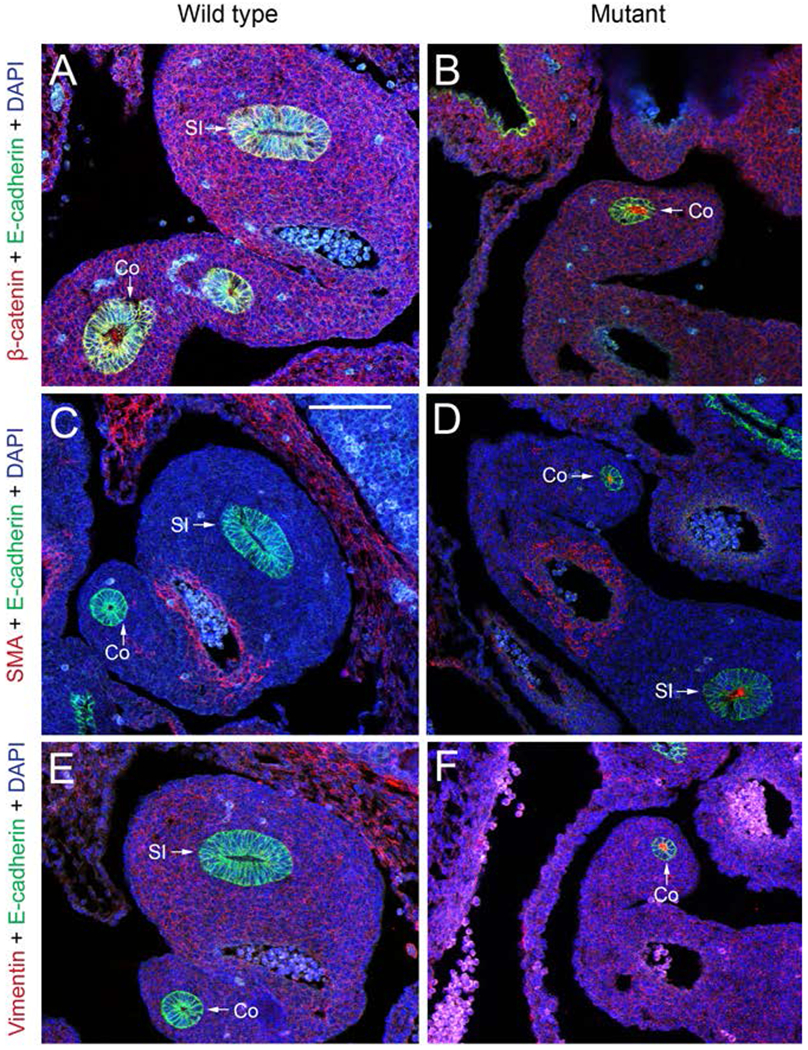
Results: We observed a global increase in intestinal epithelial apoptosis in Fgfr2IIIb -/- intestines from E9.5 to E10.5 that did not colocalize to the atretic precursor. Additionally, epithelial proliferations rates in Fgfr2IIIb -/- intestines were statistically indistinguishable to that of controls at E10.5 and E11.5. At E11.5 distal colonic epithelial cells in mutants failed to assume the expected pseudostratified columnar architecture and the continuity of the adjacent basal lamina was disrupted. Individual E-cadherin-positive cells were observed in the colonic mesenchyme.
Conclusions: Our observations suggest that alterations in proliferation and apoptosis alone are insufficient to account for intestinal atresias and that these defects may arise from both a failure of distal colonic epithelial cells to develop normally and local disruptions in basal lamina architecture.
Keywords: E-cadherin; EMT; basal lamina; embryonic development; gene expression; laminin; mice.
© 2020 Wiley Periodicals, Inc.
Figures
Similar articles
-
Formation of intestinal atresias in the Fgfr2IIIb-/- mice is not associated with defects in notochord development or alterations in Shh expression.J Surg Res. 2012 Sep;177(1):139-45. doi: 10.1016/j.jss.2012.04.024. Epub 2012 Apr 29. J Surg Res. 2012. PMID: 22572615 Free PMC article.
-
Formation of duodenal atresias in fibroblast growth factor receptor 2IIIb-/- mouse embryos occurs in the absence of an endodermal plug.J Pediatr Surg. 2012 Jul;47(7):1369-79. doi: 10.1016/j.jpedsurg.2012.02.001. J Pediatr Surg. 2012. PMID: 22813799 Free PMC article.
-
Exogenous Sonic hedgehog protein does not rescue cultured intestine from atresia formation.J Surg Res. 2014 Mar;187(1):14-8. doi: 10.1016/j.jss.2013.11.1114. Epub 2013 Dec 7. J Surg Res. 2014. PMID: 24393341 Free PMC article.
-
Haploinsufficiency of retinaldehyde dehydrogenase 2 decreases the severity and incidence of duodenal atresia in the fibroblast growth factor receptor 2IIIb-/- mouse model.Surgery. 2012 Oct;152(4):768-75; discussion 775-6. doi: 10.1016/j.surg.2012.07.022. Surgery. 2012. PMID: 23021139 Free PMC article.
-
Retinaldehyde dehydrogenase 2 is down-regulated during duodenal atresia formation in Fgfr2IIIb-/- mice.J Surg Res. 2012 Jun 1;175(1):82-7. doi: 10.1016/j.jss.2011.02.040. Epub 2011 Mar 21. J Surg Res. 2012. PMID: 21492869 Free PMC article.
Cited by
-
New developments in the biology of fibroblast growth factors.WIREs Mech Dis. 2022 Jul;14(4):e1549. doi: 10.1002/wsbm.1549. Epub 2022 Feb 9. WIREs Mech Dis. 2022. PMID: 35142107 Free PMC article. Review.
References
-
- (ICBDSR) ICFBDSAR. INTERNATIONAL CLEARINGHOUSE FOR BIRTH DEFECTS SURVEILLANCE AND RESEARCH Annual Report 2014. http://www.icbdsr.org/wp-content/annual_report/Report2014.pdf. Published 2014. Accessed September 10, 2018.
-
- Takahashi D, Hiroma T, Takamizawa S, Nakamura T. Population-based study of esophageal and small intestinal atresia/stenosis. Pediatr Int. 2014;56(6):838–844. - PubMed
-
- Dalla Vecchia LK GJ, West KW, Rescorla FJ, Scherer LR, Engum SA. Intestinal atresia and stenosis: A 25-year experience with 277 cases. Archives of Surgery. 1998;133(5):490–497. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
