

Association of pulse rate with outcomes in heart failure with reduced ejection fraction: a retrospective cohort study
- PMID: 32101141
- PMCID: PMC7045436
- DOI: 10.1186/s12872-020-01384-6
Association of pulse rate with outcomes in heart failure with reduced ejection fraction: a retrospective cohort study
Abstract
Background: In a real-world setting, the effect of pulse rate measured at the time of diagnosis and serially during follow-up and management, on outcomes in heart failure with reduced ejection fraction (HFrEF), has not been well-studied. Furthermore, how beta-blockade use in a real-world situation modifies this relation between pulse rate and outcomes in HFrEF is not well-known. Hence, we identified a large, national, real-world cohort of HFrEF to examine the association of pulse rate and outcomes.
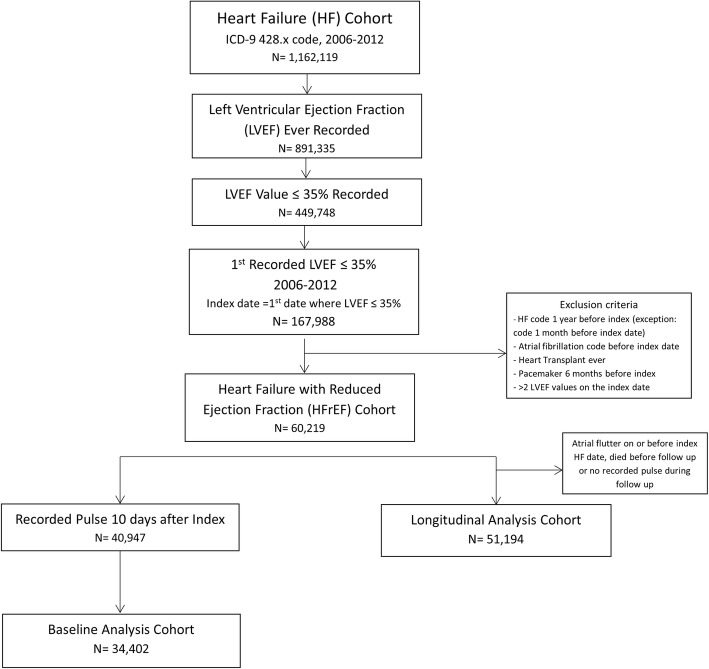
Methods: Using Veterans Affairs (VA) national electronic health records we identified incident HFrEF cases between 2006 and 2012. We examined the associations of both baseline and serially measured pulse rates, with mortality and days hospitalized per year for heart failure and for any cause, using crude and multivariable Cox proportional hazards and Poisson or negative binomial models, respectively. The exposure was examined as continuous, dichotomous, and categorical. Post-hoc analyses addressed the interaction of pulse rate and beta-blocker target dose.
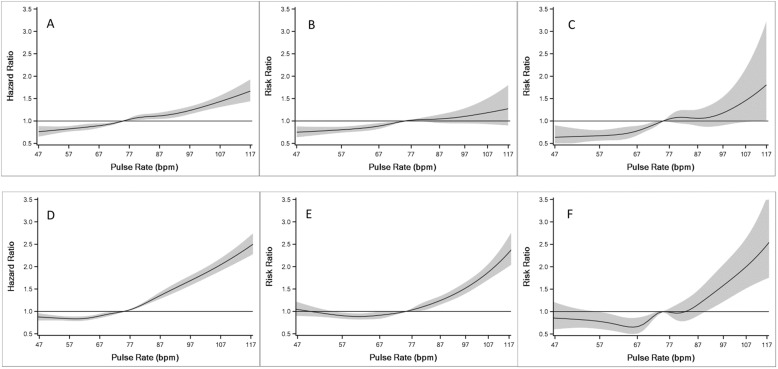
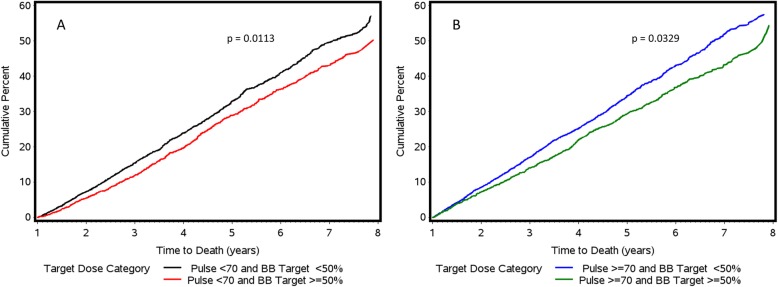
Results: We identified 51,194 incident HFrEF cases (67 ± 12 years, 98% male, 77% white. A significant positive, near linear relationship was observed for both baseline and serially measured pulse rates with all-cause mortality, all-cause hospitalization and heart failure hospitalization after adjusting for covariates including beta-blocker use. Patients who had a pulse rate ≥ 70 bpm in the past 6 months had 36% (95% CI: 31-42%), 25% (95% CI: 19-32%), and 51% (95% CI: 33-72%) increased rates of mortality, all-cause hospitalization, and heart failure hospitalization, respectively, compared to patients with pulse rates < 70 bpm. A minority of subjects (15%) were treated with guideline directed beta blockade ≥50% of recommended target dose, among whom better outcomes were seen compared to those who did not achieve target dose in patients with pulse rates both above and below 70 beats per minute.
Conclusions: High pulse rate, both at the time of diagnosis and during follow-up, is strongly associated with increased risk of adverse outcomes in HFrEF patients, independent of the use of beta-blockers. In a real-world setting, the majority of HFrEF patients do not achieve target dose of beta-blockade; greater use of strategies to reduce heart rate may improve outcomes in HFrEF.
Keywords: Beta-blocker; Heart failure; Heart rate; Hospitalization; Mortality; Outcomes.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Reil JC, Reil GH, Bohm M. Heart rate reduction by If-Channel inhibition and its potential role in heart failure with reduced and preserved ejection fraction. TCM. 2009;19(5):152–157. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
