

Effects of combined warmed preoperative forced-air and warmed perioperative intravenous fluids on maternal temperature during cesarean section: a prospective, randomized, controlled clinical trial
- PMID: 32101145
- PMCID: PMC7043061
- DOI: 10.1186/s12871-020-00970-7
Effects of combined warmed preoperative forced-air and warmed perioperative intravenous fluids on maternal temperature during cesarean section: a prospective, randomized, controlled clinical trial
Abstract
Background: Preventing the frequent perioperative hypothermia incidents that occur during elective caesarean deliveries would be beneficial. This trial aimed at evaluating the effect of preoperative forced-air warming alongside perioperative intravenous fluid warming in women undergoing cesarean sections under spinal anesthesia.
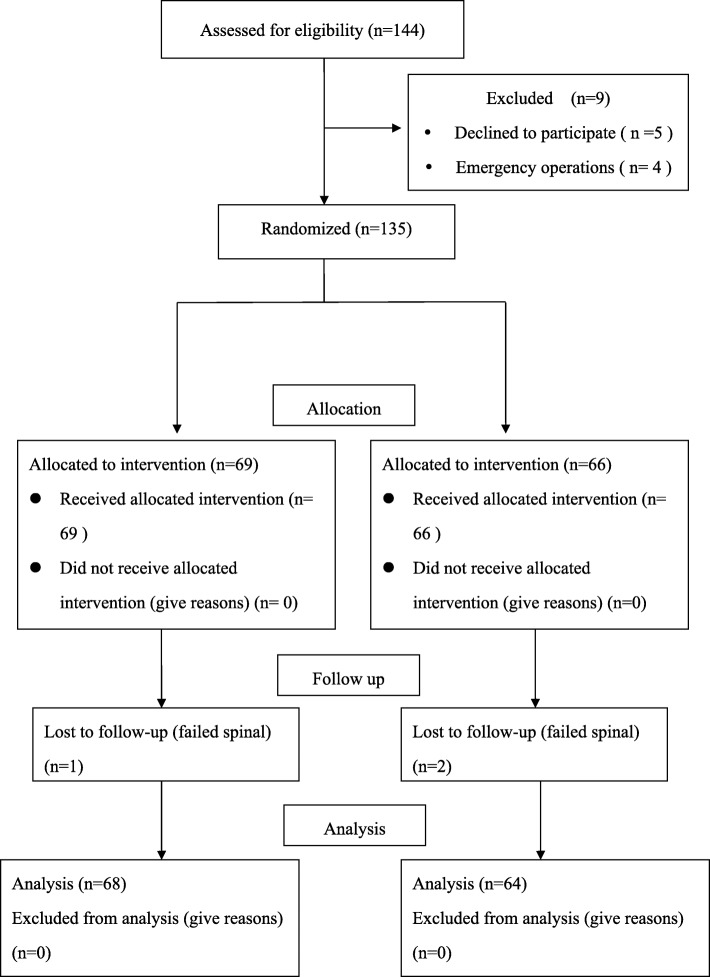
Methods: We randomly allocated 135 women undergoing elective cesarean deliveries to either the intervention group (preoperative forced-air and intravenous fluid warming, n = 69) or the control group (no active warming, n = 66). The primary outcome measure was the core temperature change between groups from baseline to the end of the surgical procedure. Secondary outcomes included thermal comfort scores, the incidences of shivering and hypothermia (< 36 °C), the core temperature on arrival at the post-anesthesia care unit, neonatal axillary temperature at birth, and Apgar scores.
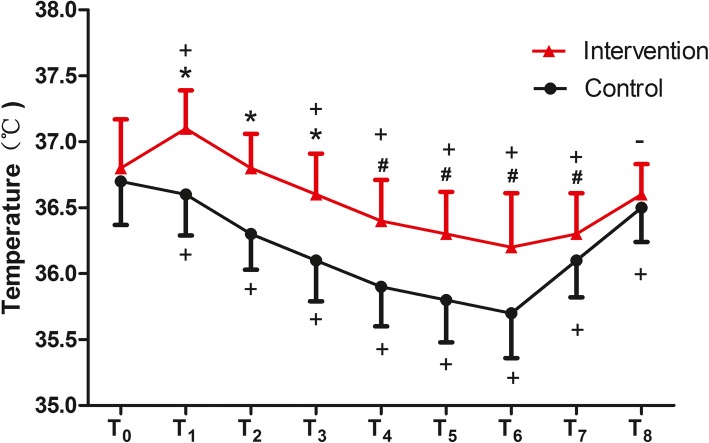
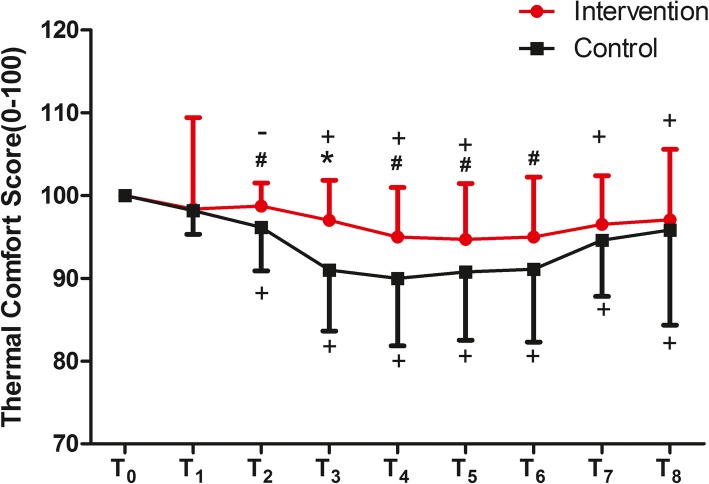
Results: Two-way repeated measures ANOVA revealed significantly different core temperature changes (from the pre-spinal temperature to that at the end of the procedure) between groups (F = 13.022, P < 0.001). The thermal comfort scores were also higher in the intervention group than in the control group (F = 9.847, P = 0.002). The overall incidence of perioperative hypothermia was significantly lower in the intervention group than in the control group (20.6% vs. 51.6%, P < 0.0001).
Conclusions: Warming preoperative forced-air and perioperative intravenous fluids may prevent maternal hypothermia, reduce maternal shivering, and improve maternal thermal comfort for patients undergoing cesarean sections under spinal anesthesia.
Trial registration: The study was registered with the Chinese Clinical Trial Registry (registration number: ChiCTR1800019117) on October26, 2018.
Keywords: Cesarean section; Spinal anesthesia; Warming.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Carpenter L, Baysinger CL. Maintaining perioperative normothermia in the patient undergoing cesarean delivery. ObstetGynecolSurv. 2012;67:436–446. - PubMed
-
- Butwick AJ, Lipman SS, Carvalho B. Intraoperative forced air-warming during cesarean delivery under spinal anesthesia does not prevent maternal hypothermia. AnesthAnalg. 2007;105:1413–1419. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
