

Effect of a Skin Self-monitoring Smartphone Application on Time to Physician Consultation Among Patients With Possible Melanoma: A Phase 2 Randomized Clinical Trial
- PMID: 32101302
- PMCID: PMC7137684
- DOI: 10.1001/jamanetworkopen.2020.0001
Effect of a Skin Self-monitoring Smartphone Application on Time to Physician Consultation Among Patients With Possible Melanoma: A Phase 2 Randomized Clinical Trial
Abstract
Importance: Melanoma is among the most lethal skin cancers; it has become the fifth most common cancer in the United Kingdom, and incidence rates are rising. Population approaches to reducing incidence have focused on mass media campaigns to promote earlier presentation and potentially improve melanoma outcomes; however, interventions using smartphone applications targeting those with the greatest risk could promote earlier presentation to health care professionals for individuals with new or changing skin lesions.
Objective: To study the effect of a commercially available skin self-monitoring (SSM) smartphone application among individuals with increased risk of melanoma on their decision to seek help for changing skin lesions.
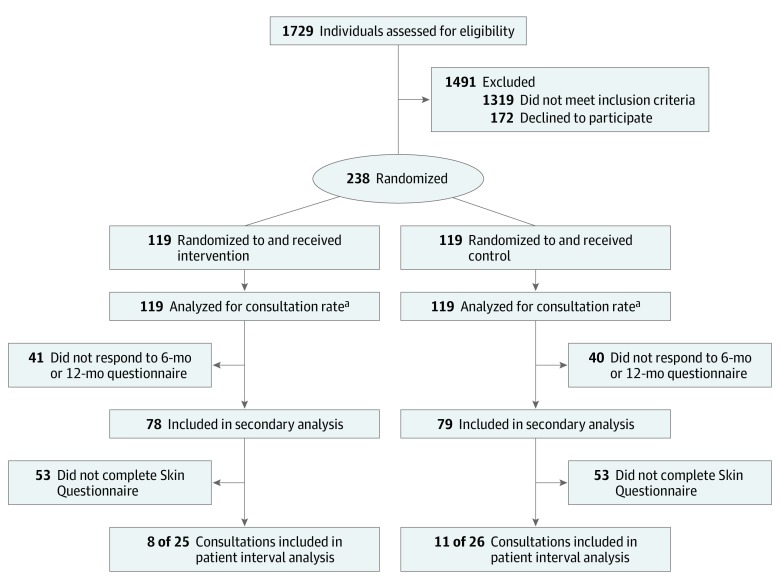
Design, setting, and participants: This phase 2 randomized clinical trial was conducted in 12 family practices in Eastern England between 2016 and 2017. A total of 238 participants, aged 18 to 75 years and with an increased risk of melanoma, were identified using a real-time melanoma risk assessment tool in family practice waiting rooms. Analysis was intention to treat. Participants were observed for 12 months, and data analysis was conducted from January to August 2018.
Intervention: The intervention and control groups received a consultation with standard written advice on sun protection and skin cancer detection. The intervention group had an SSM application loaded on their smartphone and received instructions for use and monthly self-monitoring reminders.
Main outcomes and measures: The coprimary outcomes were skin consultation rates with family practice physicians and patient intervals, measured as the time between noticing a skin change and consulting with a family practice clinician. Follow-up questionnaires were sent at 6 and 12 months, and consultation rates were extracted from family practice records. Secondary outcomes included skin self-examination benefits and barriers, self-efficacy for consulting without delay, perceived melanoma risk, sun protection habits, and potential harms.
Results: A total of 238 patients were randomized (median [interquartile range] age, 55 [43-65] years, 131 [55.0%] women, 227 [95.4%] white British; 119 [50.0%] randomized to the intervention group). Overall, 51 participants (21.4%) had consultations regarding skin changes during the 12 months of follow-up, and 157 participants (66.0%) responded to at least 1 follow-up questionnaire. There were no significant differences in skin consultation rates (adjusted risk ratio, 0.96; 95% CI, 0.56 to 1.66; P = .89), measures of SSM (adjusted mean difference, 0.08; 95% CI, -0.83 to 1.00; P = .86), or psychological harm (eg, Melanoma Worry Scale: adjusted mean difference, -0.12; 95% CI, -0.56 to 0.31; P = .58).
Conclusions and relevance: In this study, recruitment, retention, and initial delivery of the intervention were feasible, and this research provided no evidence of harm from the SSM smartphone application. However, no evidence of benefit on skin self-examination or health care consulting was found, and there is no reason at this stage to recommend its implementation in this population at increased risk of melanoma.
Trial registration: isrctn.org Identifier: ISRCTN16061621.
Conflict of interest statement
Figures
References
-
- International Agency for Research on Cancer Global Cancer Observatory. http://gco.iarc.fr/. Accessed August 5, 2019.
-
- Office for National Statistics Cancer registration statistics, England: 2016. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/.... Accessed August 5, 2019.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
