

Systematic Dementia Screening by Multidisciplinary Team Meetings in Nursing Homes for Reducing Emergency Department Transfers: The IDEM Cluster Randomized Clinical Trial
- PMID: 32101308
- PMCID: PMC7137681
- DOI: 10.1001/jamanetworkopen.2020.0049
Systematic Dementia Screening by Multidisciplinary Team Meetings in Nursing Homes for Reducing Emergency Department Transfers: The IDEM Cluster Randomized Clinical Trial
Abstract
Importance: Dementia is often underdiagnosed in nursing homes (NHs). This potentially results in inappropriate care, and high rates of emergency department (ED) transfers in particular.
Objective: To assess whether systematic dementia screening of NH residents combined with multidisciplinary team meetings resulted in a lower rate of ED transfer at 12 months compared with usual care.
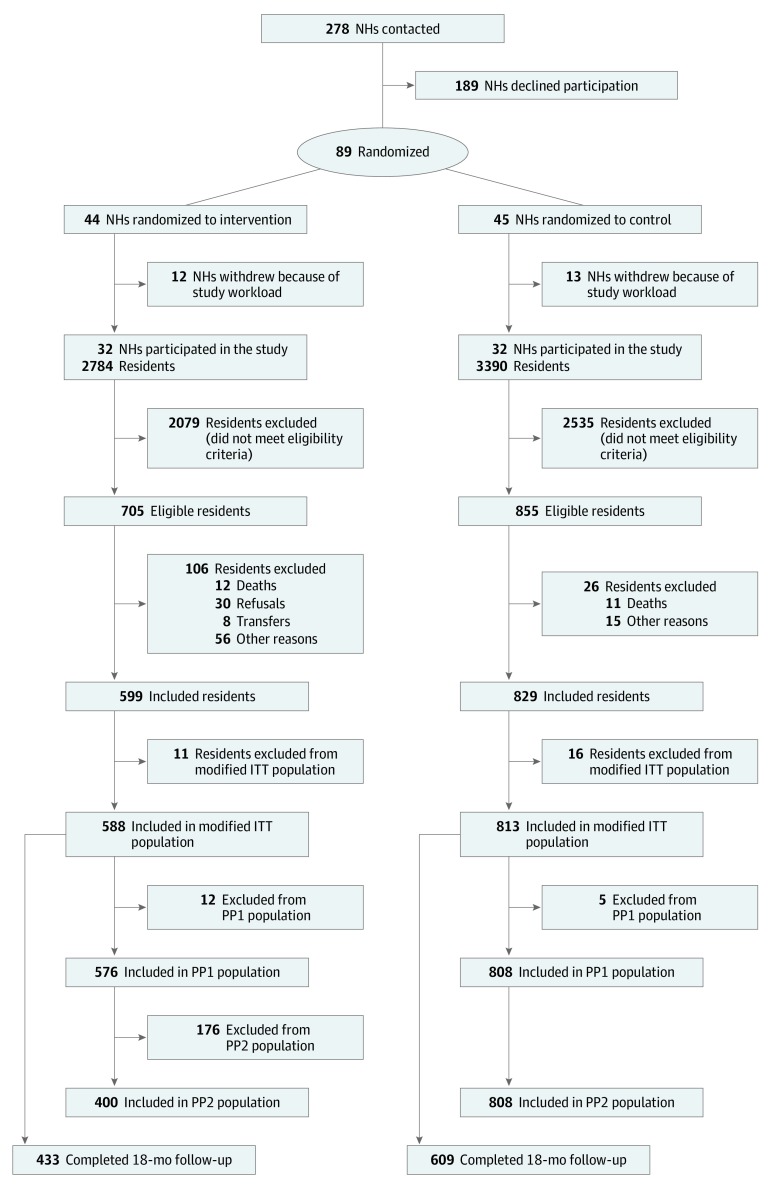
Design, setting, and participants: Multicenter, cluster randomized trial with NHs as the unit of randomization. The IDEM (Impact of Systematic Tracking of Dementia Cases on the Rate of Hospitalization in Emergency Care Units) trial took place at 64 public and private NHs in France. Recruitment started on May 1, 2010, and was completed on March 31, 2012. Residents who were aged 60 years or older, had no diagnosed or documented dementia, were not bedridden, had lived in the NH for at least 1 month at inclusion, and had a life expectancy greater than 12 months were included. The residents were followed up for 18 months. The main study analyses were completed on October 14, 2016.
Intervention: Two parallel groups were compared: an intervention group consisting of NHs that set up 2 multidisciplinary team meetings to identify residents with dementia and to discuss an appropriate care plan, and a control group consisting of NHs that continued their usual practice. During the inclusion period of 23 months, all residents of participating NHs who met eligibility criteria were included in the study.
Main outcomes and measures: The primary end point (ED transfer) was analyzed at 12 months, but the residents included were followed up for 18 months.
Results: A total of 64 NHs participated in the study and enrolled 1428 residents (mean [SD] age, 84.7 [8.1] years; 1019 [71.3%] female): 599 in the intervention group (32 NHs) and 829 in the control group (32 NHs). The final study visit was completed by 1042 residents (73.0%). The main reason for early discontinuation was death (318 residents [22.7%]). The intervention did not reduce the risk of ED transfers during the 12-month follow-up: the proportion of residents transferred at least once to an ED during the 12-month follow-up was 16.2% in the intervention group vs 12.8% in the control group (odds ratio, 1.32; 95% CI, 0.83-2.09; P = .24).
Conclusions and relevance: This study failed to demonstrate that systematic screening for dementia in NHs resulted in fewer ED transfers. The findings do not support implementation of multidisciplinary team meetings for systematic dementia screening of all NH residents, beyond the national recommendations for dementia diagnosis, to reduce ED transfers.
Trial registration: ClinicalTrials.gov Identifier: NCT01569997.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
