

Impact of hyperthyroidism on cardiac hypertrophy
- PMID: 32101527
- PMCID: PMC7159257
- DOI: 10.1530/EC-19-0543
Impact of hyperthyroidism on cardiac hypertrophy
Abstract
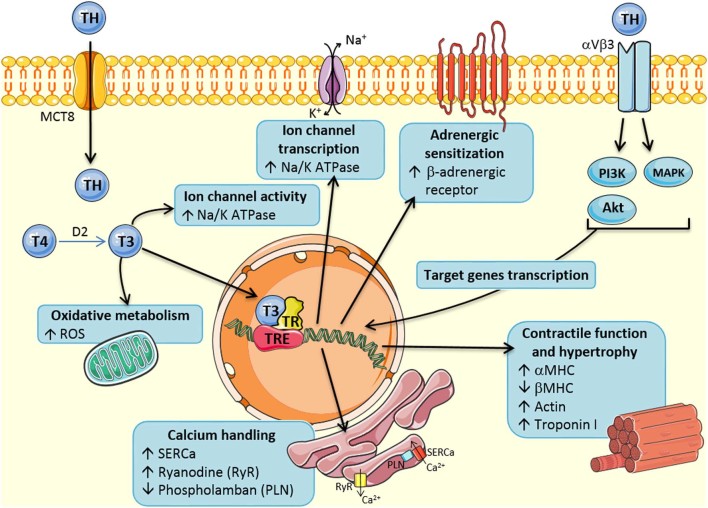
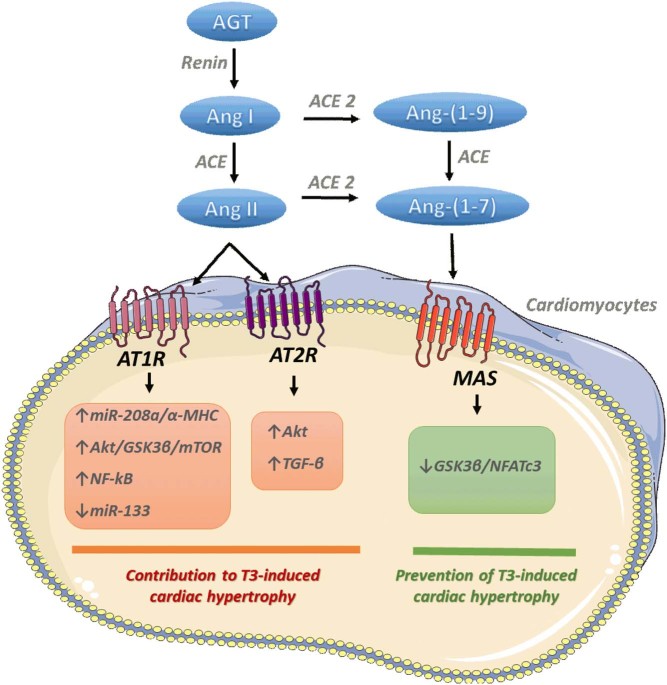
The cardiac growth process (hypertrophy) is a crucial phenomenon conserved across a wide array of species and is critically involved in the maintenance of cardiac homeostasis. This process enables an organism to adapt to changes in systemic demand and occurs due to a plethora of responses, depending on the type of signal or stimuli received. The growth of cardiac muscle cells in response to environmental conditions depends on the type, strength and duration of stimuli, and results in adaptive physiological responses or non-adaptive pathological responses. Thyroid hormones (TH) have a direct effect on the heart and induce a cardiac hypertrophy phenotype, which may evolve to heart failure. In this review, we summarize the literature on TH function in the heart by presenting results from experimental studies. We discuss the mechanistic aspects of TH associated with cardiac myocyte hypertrophy, increased cardiac myocyte contractility and electrical remodeling, as well as the associated signaling pathways. In addition to classical crosstalk with the sympathetic nervous system (SNS), emerging work pointing to the new endocrine interaction between TH and the renin-angiotensin system (RAS) is also explored. Given the inflammatory potential of the angiotensin II peptide, this new interaction may open the door for new therapeutic approaches which target the key mechanisms responsible for TH-induced cardiac hypertrophy.
Keywords: cardiac myocyte; cardiac remodeling; molecular mechanisms; renin-angiotensin system; thyroid hormones.
Figures
Similar articles
-
The renin-angiotensin system and experimental heart failure.Cardiovasc Res. 1999 Sep;43(4):838-49. doi: 10.1016/s0008-6363(99)00145-5. Cardiovasc Res. 1999. PMID: 10615411 Review.
-
TRP Channels in the Heart.In: Emir TLR, editor. Neurobiology of TRP Channels. Boca Raton (FL): CRC Press/Taylor & Francis; 2017. Chapter 9. In: Emir TLR, editor. Neurobiology of TRP Channels. Boca Raton (FL): CRC Press/Taylor & Francis; 2017. Chapter 9. PMID: 29356479 Free Books & Documents. Review.
-
AT1 receptor blockage impairs NF-κB activation mediated by thyroid hormone in cardiomyocytes.Pflugers Arch. 2018 Mar;470(3):549-558. doi: 10.1007/s00424-017-2088-6. Epub 2017 Nov 25. Pflugers Arch. 2018. PMID: 29178049
-
Thyroxine-induced cardiac hypertrophy: influence of adrenergic nervous system versus renin-angiotensin system on myocyte remodeling.Am J Physiol Regul Integr Comp Physiol. 2003 Dec;285(6):R1473-80. doi: 10.1152/ajpregu.00269.2003. Epub 2003 Aug 21. Am J Physiol Regul Integr Comp Physiol. 2003. PMID: 12933361
-
Cardiac microRNA-133 is down-regulated in thyroid hormone-mediated cardiac hypertrophy partially via Type 1 Angiotensin II receptor.Basic Res Cardiol. 2015 Sep;110(5):49. doi: 10.1007/s00395-015-0504-7. Epub 2015 Jul 23. Basic Res Cardiol. 2015. PMID: 26202011
Cited by
-
SARS-CoV-2 plays a pivotal role in inducing hyperthyroidism of Graves' disease.Endocrine. 2021 Aug;73(2):243-254. doi: 10.1007/s12020-021-02770-6. Epub 2021 Jun 9. Endocrine. 2021. PMID: 34106438 Free PMC article. Review.
-
Protective Effects of Thyroid Hormone Deprivation on Progression of Maladaptive Cardiac Hypertrophy and Heart Failure.Front Cardiovasc Med. 2021 Jul 30;8:683522. doi: 10.3389/fcvm.2021.683522. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34395557 Free PMC article.
-
Impact of thyroid hormone perturbations in adult mice: brain weight and blood vessel changes, gene expression variation, and neurobehavioral outcomes.Neurobiol Aging. 2023 Aug;128:74-84. doi: 10.1016/j.neurobiolaging.2023.04.012. Epub 2023 Apr 29. Neurobiol Aging. 2023. PMID: 37229849 Free PMC article.
-
Identification of atrial-enriched lncRNA Walras linked to cardiomyocyte cytoarchitecture and atrial fibrillation.FASEB J. 2022 Jan;36(1):e22051. doi: 10.1096/fj.202100844RR. FASEB J. 2022. PMID: 34861058 Free PMC article.
-
Cardiac hypertrophy that affects hyperthyroidism occurs independently of the NLRP3 inflammasome.Pflugers Arch. 2024 Jul;476(7):1065-1075. doi: 10.1007/s00424-024-02965-6. Epub 2024 Apr 29. Pflugers Arch. 2024. PMID: 38679646
References
-
- Kapitola J, Vilimovská D. Inhibition of the early circulatory effects of triiodothyronine in rats by propranolol. Physiologia Bohemoslovaca 1981. 30 347–351. (available at: http://europepmc.org/abstract/med/6458055) - PubMed
Publication types
LinkOut - more resources
Full Text Sources
