

Microbiota as Predictor of Mortality in Allogeneic Hematopoietic-Cell Transplantation
- PMID: 32101664
- PMCID: PMC7534690
- DOI: 10.1056/NEJMoa1900623
Microbiota as Predictor of Mortality in Allogeneic Hematopoietic-Cell Transplantation
Abstract
Background: Relationships between microbiota composition and clinical outcomes after allogeneic hematopoietic-cell transplantation have been described in single-center studies. Geographic variations in the composition of human microbial communities and differences in clinical practices across institutions raise the question of whether these associations are generalizable.
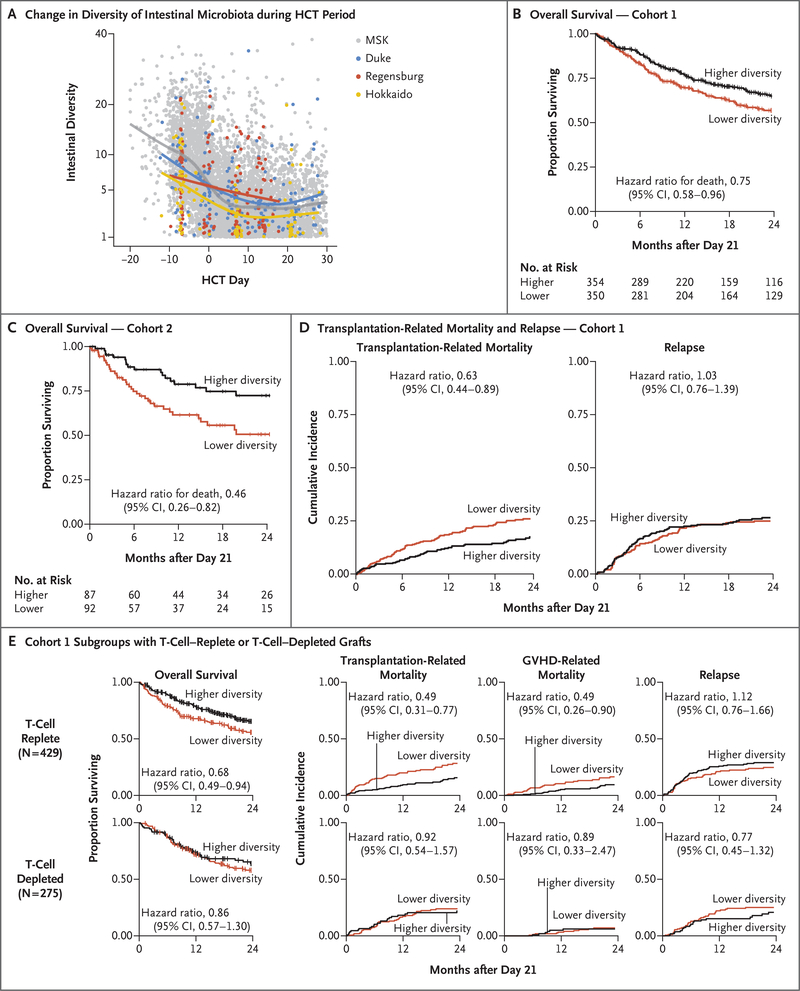
Methods: The microbiota composition of fecal samples obtained from patients who were undergoing allogeneic hematopoietic-cell transplantation at four centers was profiled by means of 16S ribosomal RNA gene sequencing. In an observational study, we examined associations between microbiota diversity and mortality using Cox proportional-hazards analysis. For stratification of the cohorts into higher- and lower-diversity groups, the median diversity value that was observed at the study center in New York was used. In the analysis of independent cohorts, the New York center was cohort 1, and three centers in Germany, Japan, and North Carolina composed cohort 2. Cohort 1 and subgroups within it were analyzed for additional outcomes, including transplantation-related death.
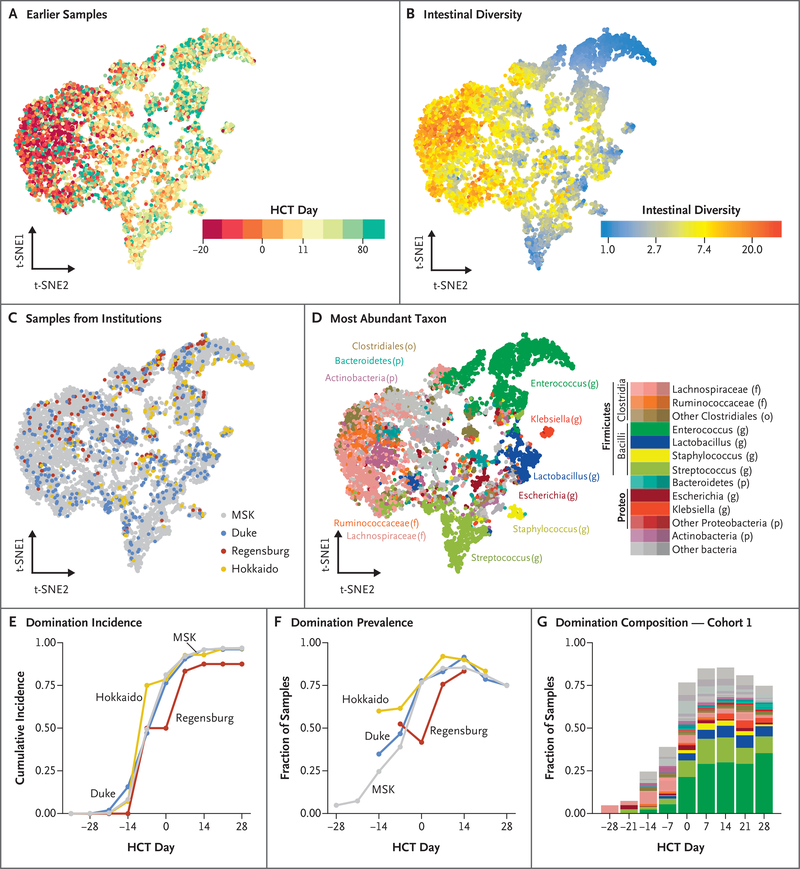
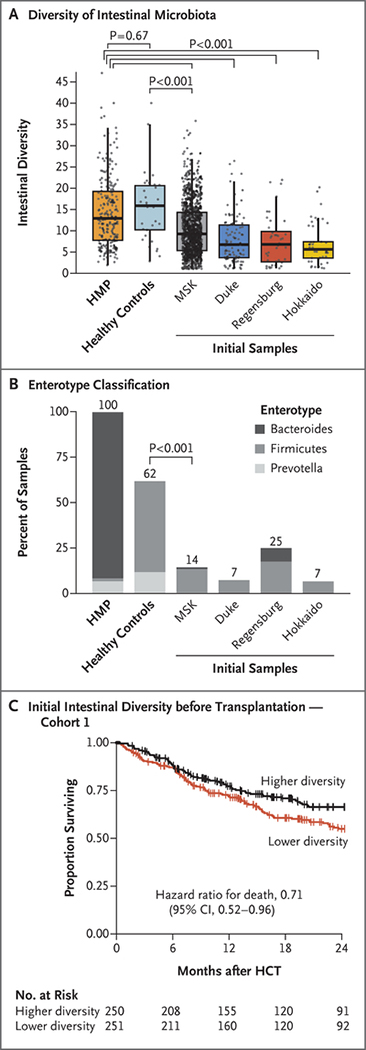
Results: We profiled 8767 fecal samples obtained from 1362 patients undergoing allogeneic hematopoietic-cell transplantation at the four centers. We observed patterns of microbiota disruption characterized by loss of diversity and domination by single taxa. Higher diversity of intestinal microbiota was associated with a lower risk of death in independent cohorts (cohort 1: 104 deaths among 354 patients in the higher-diversity group vs. 136 deaths among 350 patients in the lower-diversity group; adjusted hazard ratio, 0.71; 95% confidence interval [CI], 0.55 to 0.92; cohort 2: 18 deaths among 87 patients in the higher-diversity group vs. 35 deaths among 92 patients in the lower-diversity group; adjusted hazard ratio, 0.49; 95% CI, 0.27 to 0.90). Subgroup analyses identified an association between lower intestinal diversity and higher risks of transplantation-related death and death attributable to graft-versus-host disease. Baseline samples obtained before transplantation already showed evidence of microbiome disruption, and lower diversity before transplantation was associated with poor survival.
Conclusions: Patterns of microbiota disruption during allogeneic hematopoietic-cell transplantation were similar across transplantation centers and geographic locations; patterns were characterized by loss of diversity and domination by single taxa. Higher diversity of intestinal microbiota at the time of neutrophil engraftment was associated with lower mortality. (Funded by the National Cancer Institute and others.).
Copyright © 2020 Massachusetts Medical Society.
Figures
Comment in
-
Intestinal microbiota predict HSCT outcome.Nat Rev Clin Oncol. 2020 May;17(5):275. doi: 10.1038/s41571-020-0351-9. Nat Rev Clin Oncol. 2020. PMID: 32203272 No abstract available.
-
Microbiota and Allogeneic Hematopoietic-Cell Transplantation.N Engl J Med. 2020 Jun 11;382(24):2378. doi: 10.1056/NEJMc2006694. N Engl J Med. 2020. PMID: 32521144 No abstract available.
References
-
- Holler E, Butzhammer P, Schmid K, et al. Metagenomic analysis of the stool microbiome in patients receiving allogeneic stem cell transplantation: loss of diversity is associated with use of systemic antibiotics and more pronounced in gastrointestinal graft-versus-host disease. Biol Blood Marrow Transplant 2014;20:640–5. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- 1R01CA228308-01/CA/NCI NIH HHS/United States
- P01-AG052359 (Project 2)/AG/NIA NIH HHS/United States
- P01 CA023766/CA/NCI NIH HHS/United States
- R01 CA228308/CA/NCI NIH HHS/United States
- R01 AI137269-01/National Institute of Allergy and Infectious Diseases/International
- K08HL143189-01A1/HL/NHLBI NIH HHS/United States
- UL1 TR002553/TR/NCATS NIH HHS/United States
- P30 AG028716/AG/NIA NIH HHS/United States
- P01-CA023766 (Project 4)/CA/NCI NIH HHS/United States
- KL2 TR001115-03/TR/NCATS NIH HHS/United States
- 17K09945/Japan Society for the Promotion of Science/International
- 17H04206/Japan Society for the Promotion of Science/International
- 2016-013/US/United States/United States
- R01 HL124112/HL/NHLBI NIH HHS/United States
- 1R01HL124112-01A/HL/NHLBI NIH HHS/United States
- R01 AI032135/AI/NIAID NIH HHS/United States
- U01 AI124275/AI/NIAID NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- R01CA203950-01/CA/NCI NIH HHS/United States
- R01 AI095706/AI/NIAID NIH HHS/United States
- KL2 TR001115/TR/NCATS NIH HHS/United States
- R01-HL125571/HL/NHLBI NIH HHS/United States
- P30 CA014236/CA/NCI NIH HHS/United States
- R01-HL125571/CA/NCI NIH HHS/United States
- R01 AI100288/AI/NIAID NIH HHS/United States
- T32 AI100851/AI/NIAID NIH HHS/United States
- U01 AI124275/CA/NCI NIH HHS/United States
- K08 HL143189/HL/NHLBI NIH HHS/United States
- R01 CA203950/CA/NCI NIH HHS/United States
- R01-HL123340/HL/NHLBI NIH HHS/United States
- 2P30AG028716-11/AG/NIA NIH HHS/United States
- R01 AI032135/NH/NIH HHS/United States
- R01 AI137269/AI/NIAID NIH HHS/United States
- 1R01CA228358-01/CA/NCI NIH HHS/United States
- AI095706/National Institute of Allergy and Infectious Diseases/International
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical