

Hyperprogression and Immunotherapy: Fact, Fiction, or Alternative Fact?
- PMID: 32101722
- PMCID: PMC9726601
- DOI: 10.1016/j.trecan.2020.01.005
Hyperprogression and Immunotherapy: Fact, Fiction, or Alternative Fact?
Abstract
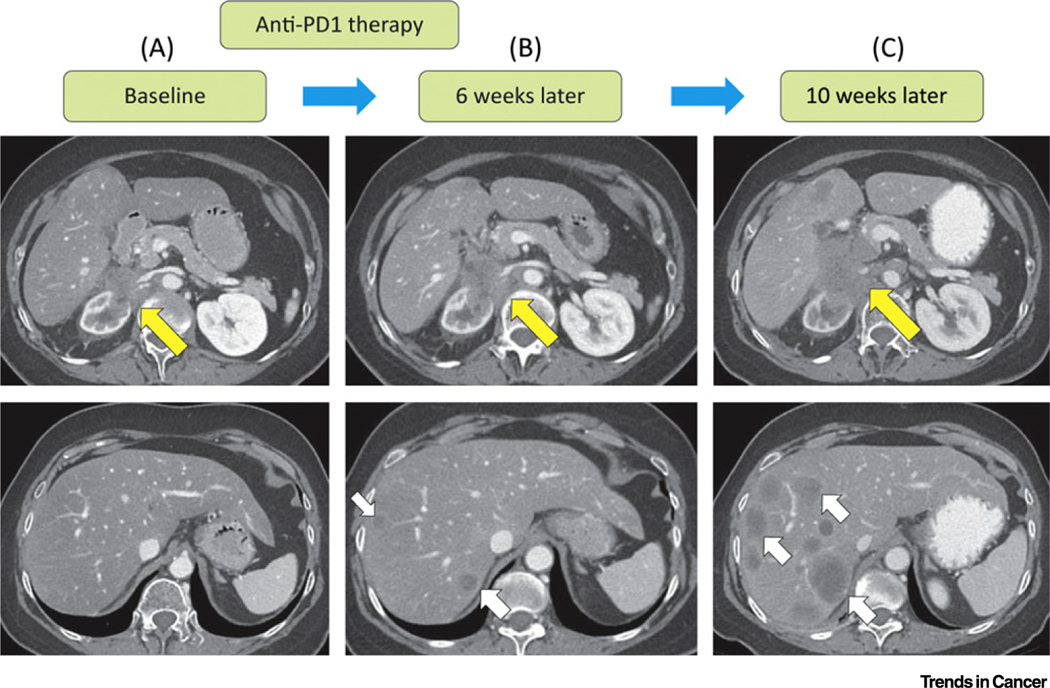
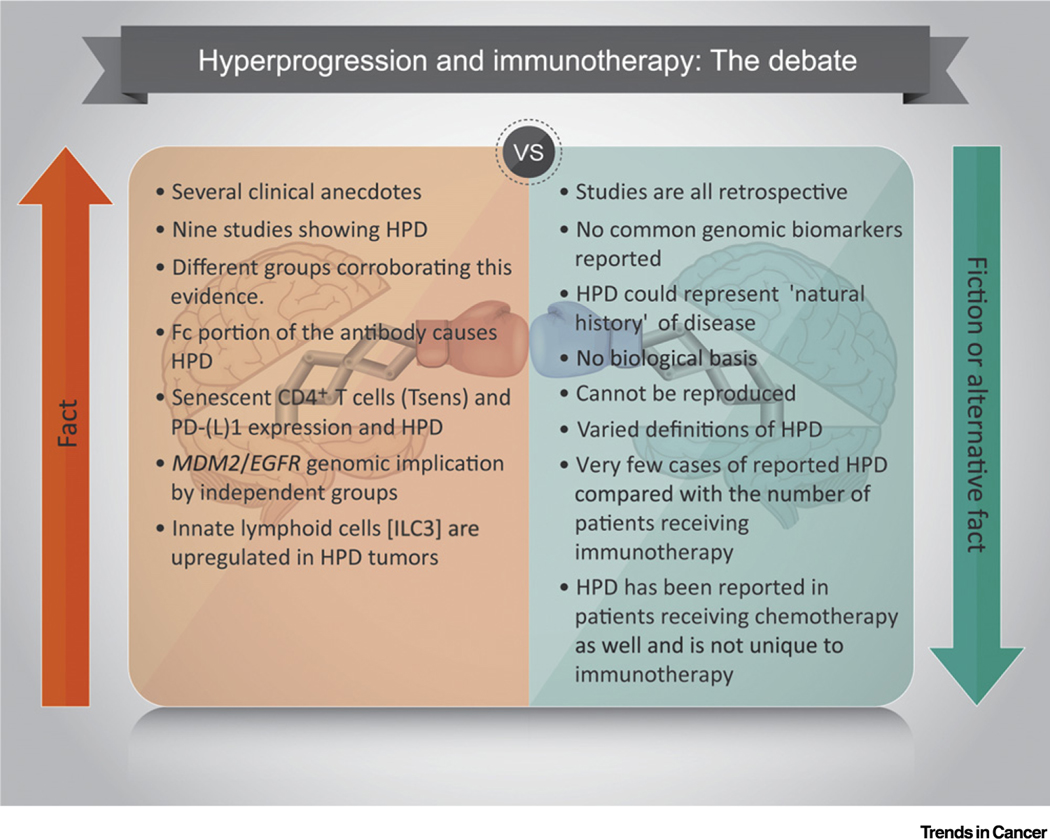
Immunotherapy (IO) has altered the therapeutic landscape for multiple cancers. There are emerging data from retrospective studies on a subset of patients who do not benefit from IO, instead experiencing rapid progression with dramatic acceleration of disease trajectory, termed 'hyperprogressive disease' (HPD). The incidence of HPD ranges from 4% to 29% from the studies reported. Biological basis and mechanisms of HPD are currently being elucidated, with one theory involving the Fc region of antibodies. Another group has shown EGFR and MDM2/MDM4 amplifications in patients with HPD. This phenomenon has polarized oncologists who debate that this could still reflect the natural history of the disease. Thus, prospective studies are urgently needed to confirm the underlying biology, predict patients who are susceptible to HPD, and determine the modality of therapy post progression.
Keywords: cancer clinical trials; hyperprogressive disease; immune checkpoint inhibitors; immunotherapy.
Copyright © 2020 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Champiat S. et al. (2017) Hyperprogressive disease is a new pattern of progression in cancer patients treated by anti-PD-1/PD-L1. Clin. Cancer Res 23, 1920–1928 - PubMed
-
- Kanjanapan Y. et al. (2018) Hyperprogressive disease (HPD) in early-phase immunotherapy (IO) trials. J. Clin. Oncol 36, 3063
-
- Matos I. et al. (2018) Incidence and clinical implications of a new definition of hyperprogression (HPD) with immune checkpoint inhibitors (ICIs) in patients treated in phase 1 (Ph1) trials. J. Clin. Oncol 36, 3032
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
