

Fractional Flow Reserve Derived from Coronary Computed Tomography Angiography Safely Defers Invasive Coronary Angiography in Patients with Stable Coronary Artery Disease
- PMID: 32102371
- PMCID: PMC7074264
- DOI: 10.3390/jcm9020604
Fractional Flow Reserve Derived from Coronary Computed Tomography Angiography Safely Defers Invasive Coronary Angiography in Patients with Stable Coronary Artery Disease
Abstract
Objectives: In the United States, the real-world feasibility and outcome of using fractional flow reserve from coronary computed tomography angiography (FFRCT) is unknown. We sought to determine whether a strategy that combined coronary computed tomography angiography (CTA) and FFRCT could safely reduce the need for invasive coronary angiography (ICA), as compared to coronary CTA alone.
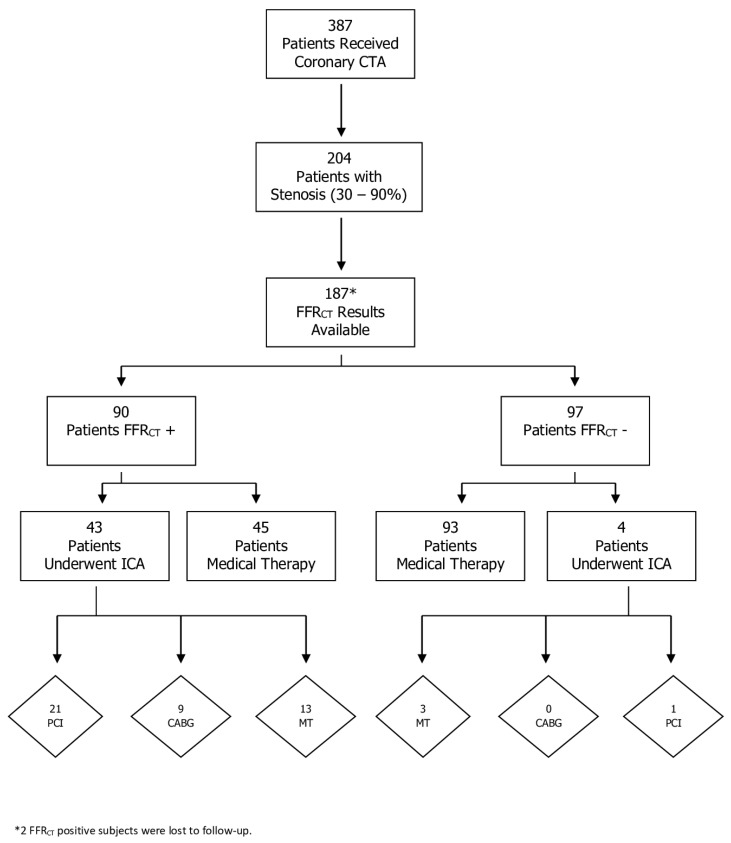
Methods: The study included 387 consecutive patients with suspected CAD referred for coronary CTA with selective FFRCT and 44 control patients who underwent CTA alone. Lesions with 30-90% diameter stenoses were considered of indeterminate hemodynamic significance and underwent FFRCT. Nadir FFRCT ≤ 0.80 was positive. The rate of patients having ICA, revascularization and major adverse cardiac events were recorded.
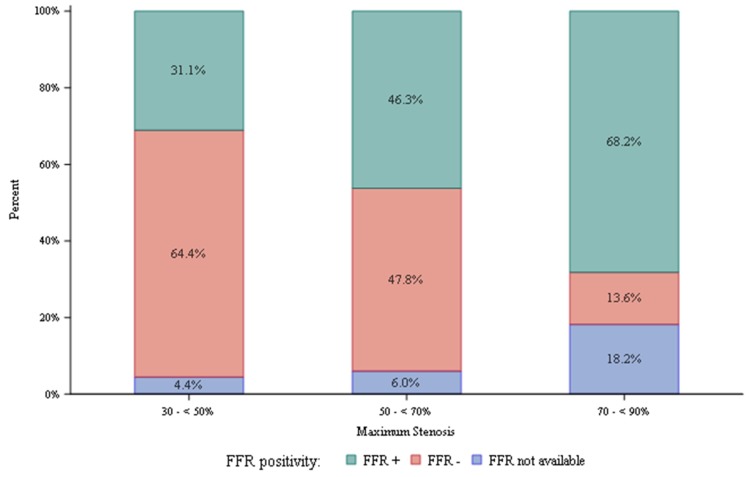
Results: Using coronary CTA and selective FFRCT, 121 patients (32%) had at least one vessel with ≥50% diameter stenosis; 67/121 (55%) patients had at least one vessel with FFRCT ≤ 0.80; 55/121 (45%) underwent ICA; and 34 were revascularized. The proportion of ICA patients undergoing revascularization was 62% (34 of 55). The number of patients with vessels with 30-50% diameter of stenosis was 90 (23%); 28/90 (31%) patients had at least one vessel with FFRCT ≤ 0.80; 8/90 (9%) underwent ICA; and five were revascularized. In our institutional practice, compared to coronary CTA alone, coronary CTA with selective FFRCT reduced the rates of ICA (45% vs. 80%) for those with obstructive CAD. Using coronary CTA with selective FFRCT, no major adverse cardiac events occurred over a mean follow-up of 440 days.
Conclusion: FFRCT safely deferred ICA in patients with CAD of indeterminate hemodynamic significance. A high proportion of those who underwent ICA were revascularized.
Keywords: computational fluid dynamics; coronary computed tomography angiography; fractional flow reserve; stable coronary artery disease.
Conflict of interest statement
M.R.: Consultant, HeartFlow; J.L.: Consultant, HeartFlow; J.B.: none; B.K.: none; S.A.: none; D.D.: none; R.V.: none; G.P.: Research grants, HeartFlow; D.W.: none; V.M.: none; C.R.: Employee, HeartFlow; J.L.: none.
Figures
References
-
- Patel M.R., Dai D., Hernandez A.F., Douglas P.S., Messenger J., Garratt K.N., Maddox T.M., Peterson E.D., Roe M.T. Prevalence and predictors of nonobstructive coronary artery disease identified with coronary angiography in contemporary clinical practice. Am. Heart J. 2014;167:846–852. doi: 10.1016/j.ahj.2014.03.001. - DOI - PubMed
-
- Vavalle J.P., Shen L., Broderick S., Shaw L.K., Douglas P.S. Effect of the Presence and Type of Angina on Cardiovascular Events in Patients Without Known Coronary Artery Disease Referred for Elective Coronary Angiography. JAMA Cardiol. 2016;1:232–234. doi: 10.1001/jamacardio.2016.0076. - DOI - PubMed
-
- Budoff M.J., Dowe D., Jollis J.G., Gitter M., Sutherland J., Halamert E., Scherer M., Bellinger R., Martin A., Benton R., et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: Results from the prospective multicenter ACCURACY (Assessment by Coro. J. Am. Coll. Cardiol. 2008;52:1724–1732. doi: 10.1016/j.jacc.2008.07.031. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
