

Cardiac Myosin Promotes Thrombin Generation and Coagulation In Vitro and In Vivo
- PMID: 32102568
- PMCID: PMC7135739
- DOI: 10.1161/ATVBAHA.120.313990
Cardiac Myosin Promotes Thrombin Generation and Coagulation In Vitro and In Vivo
Abstract
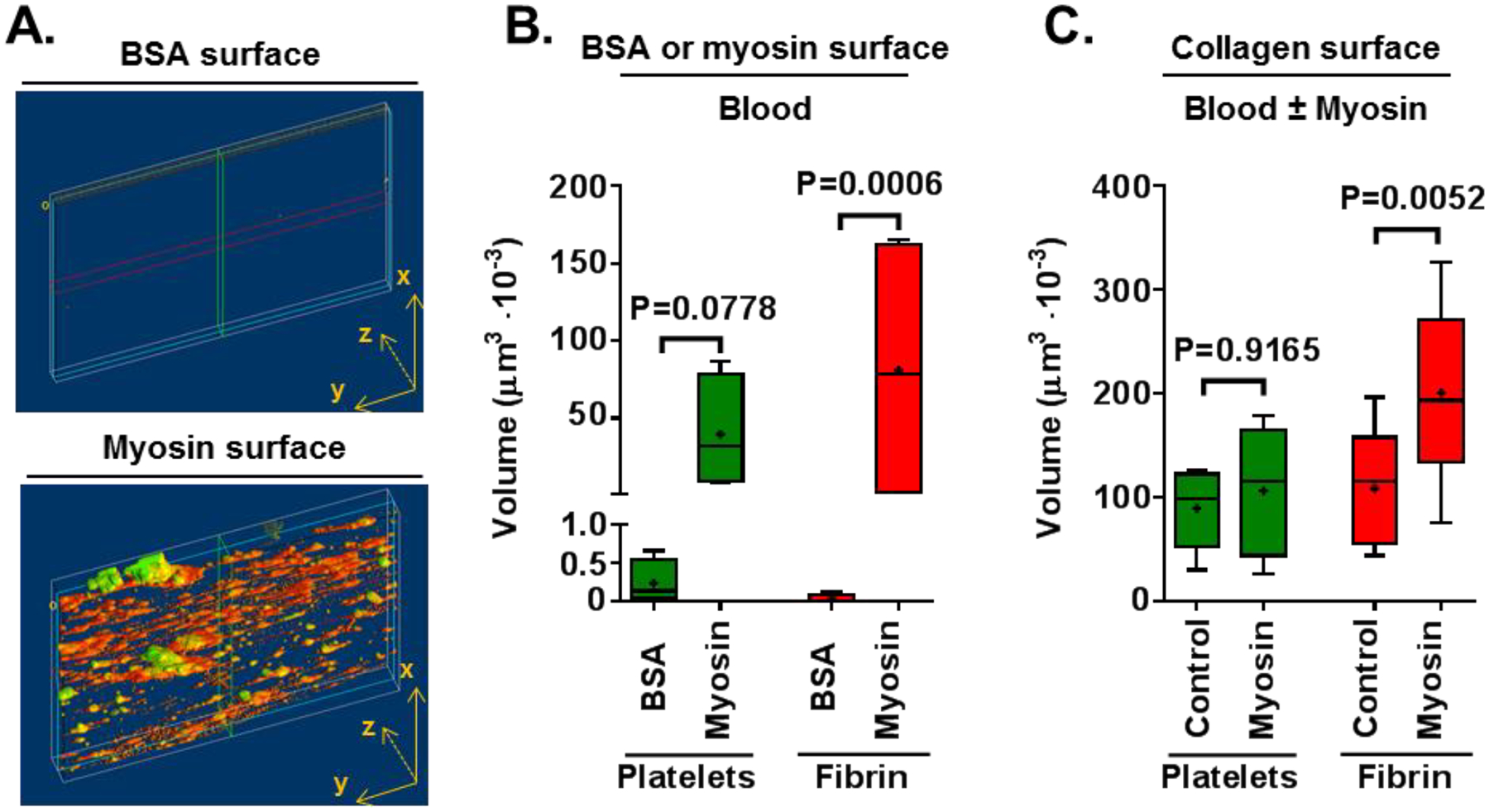
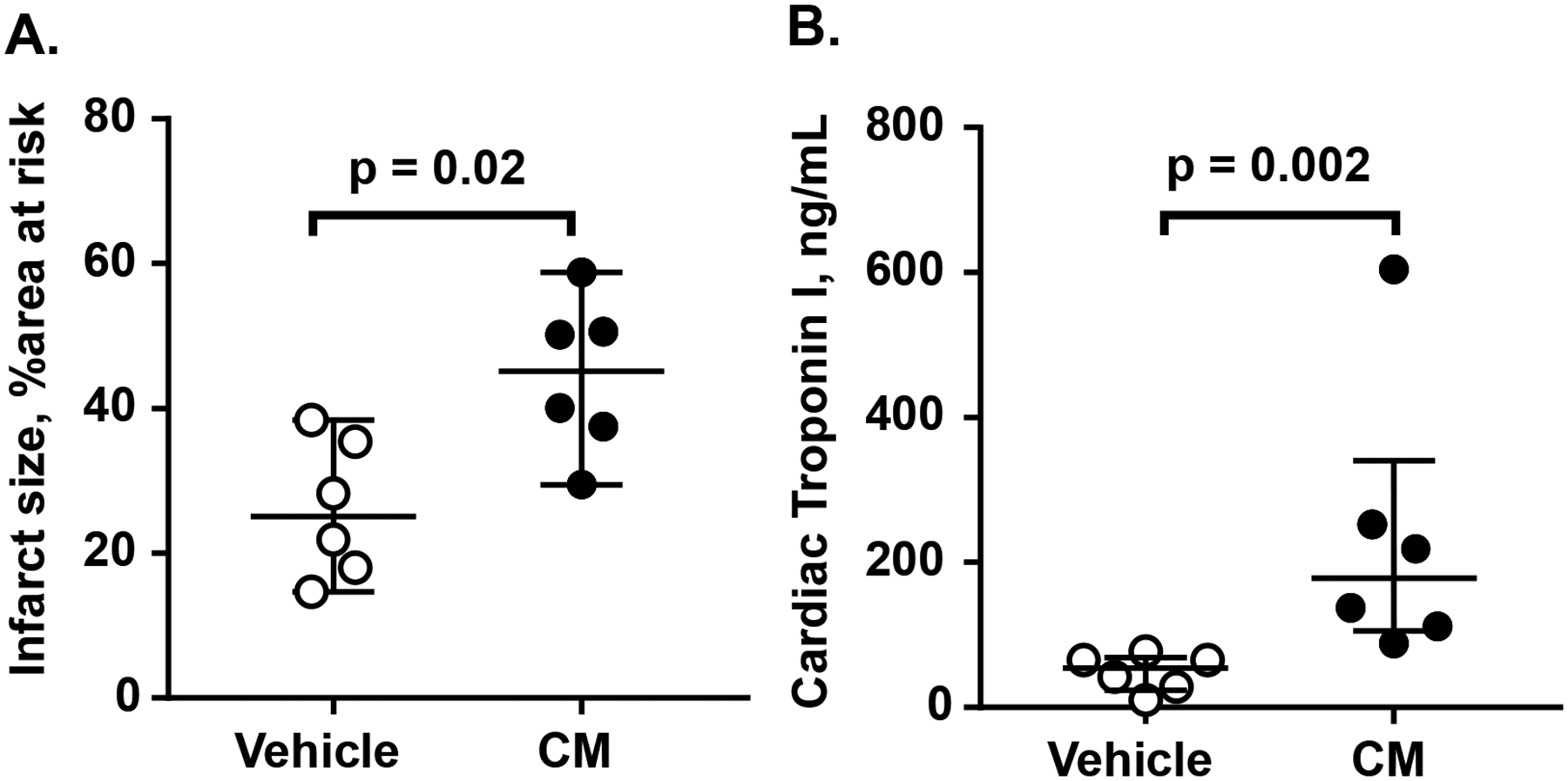
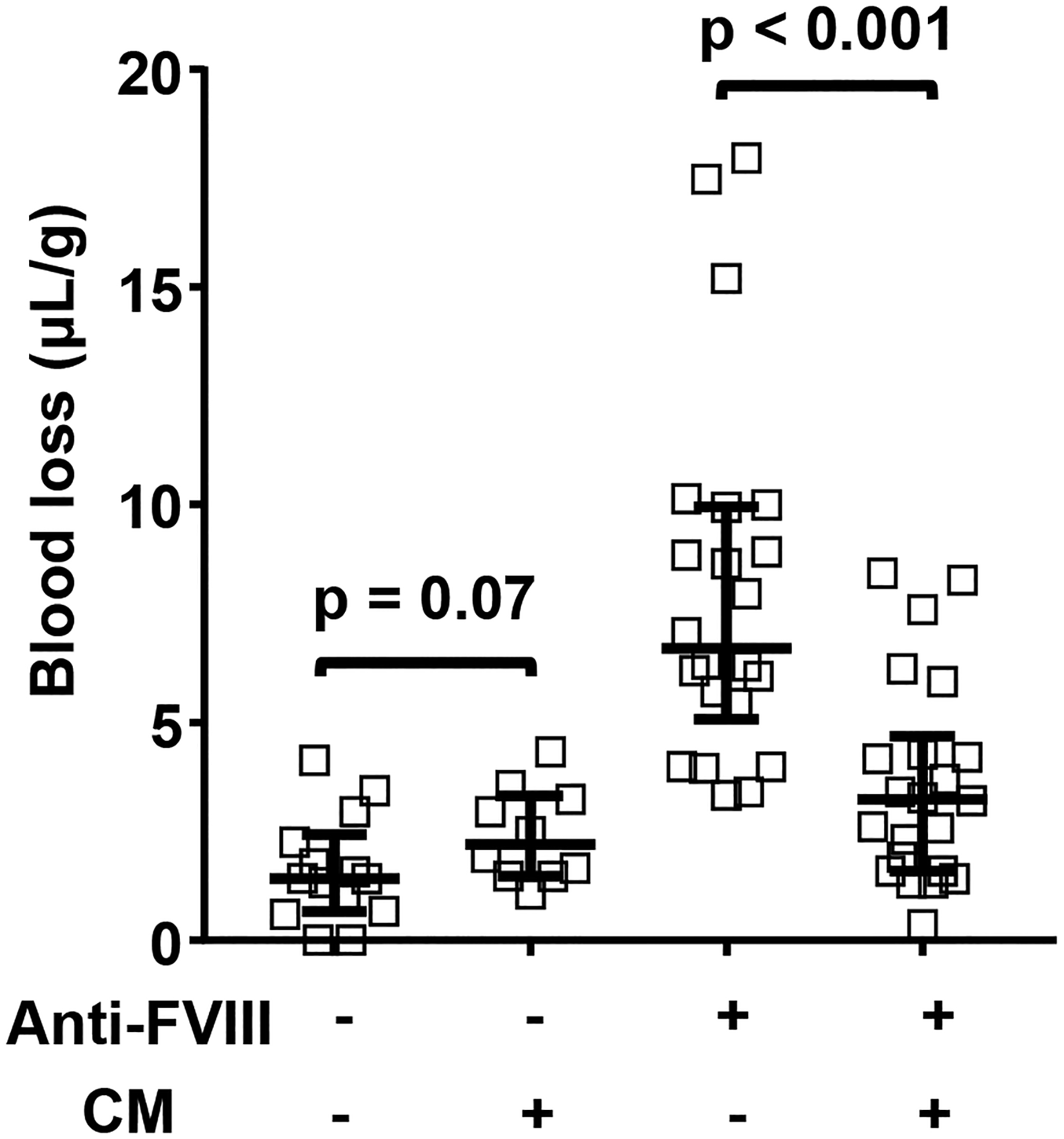
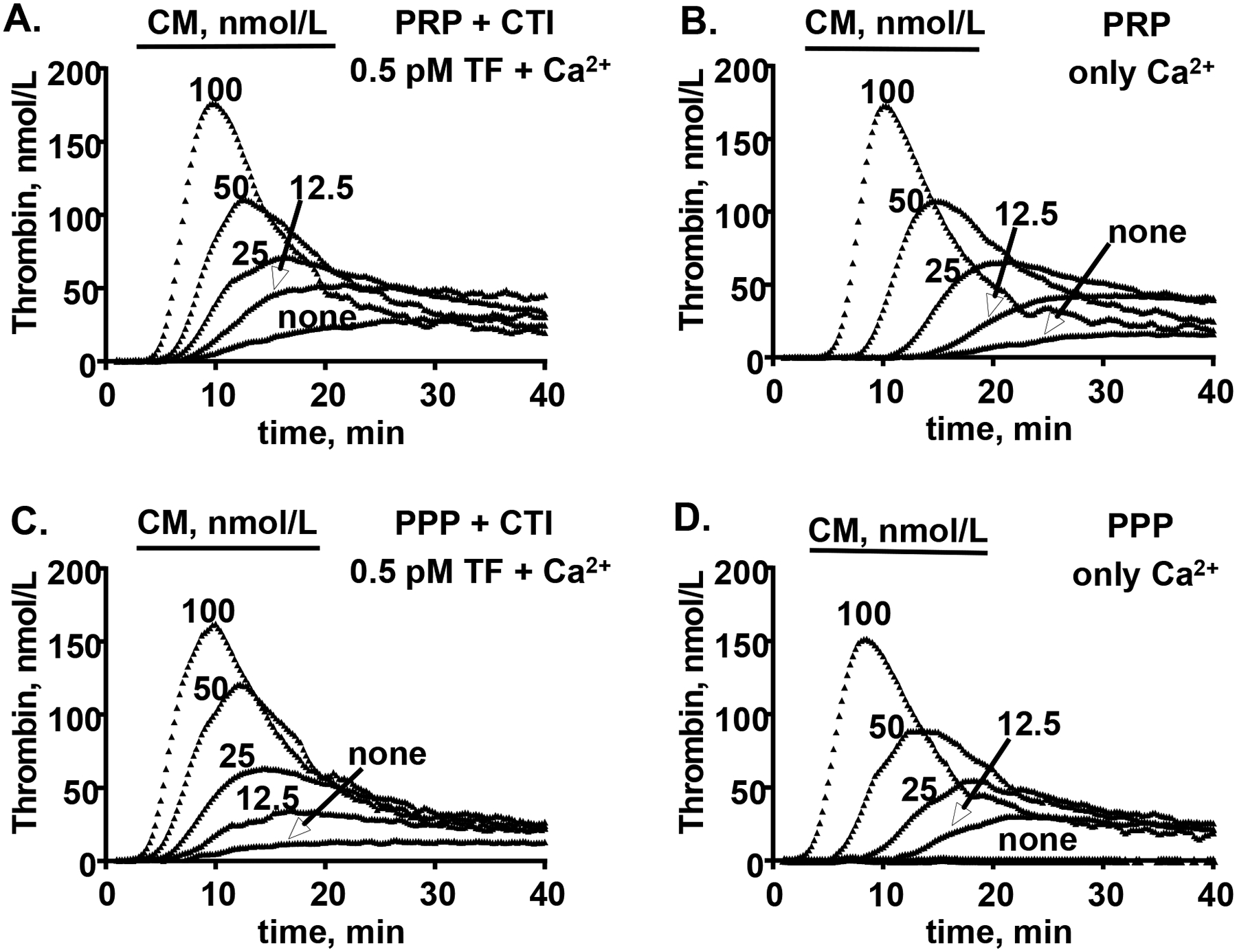
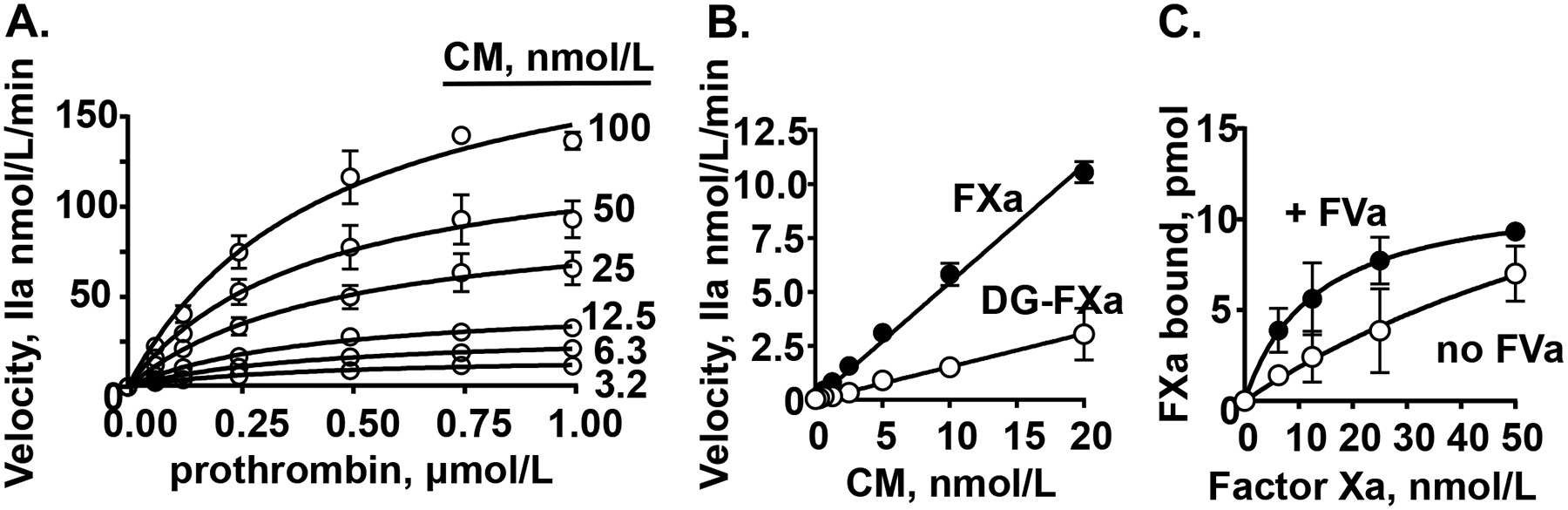
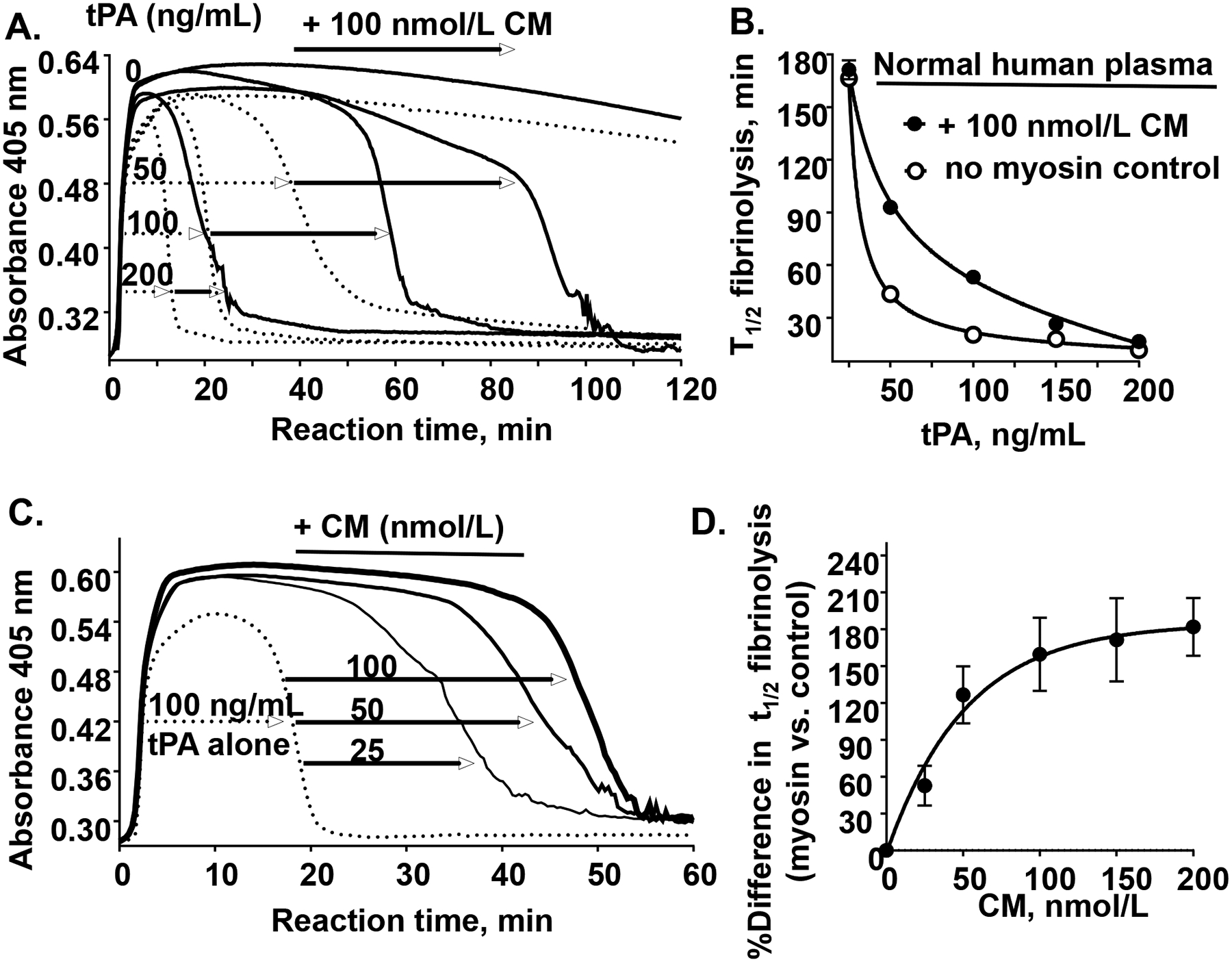
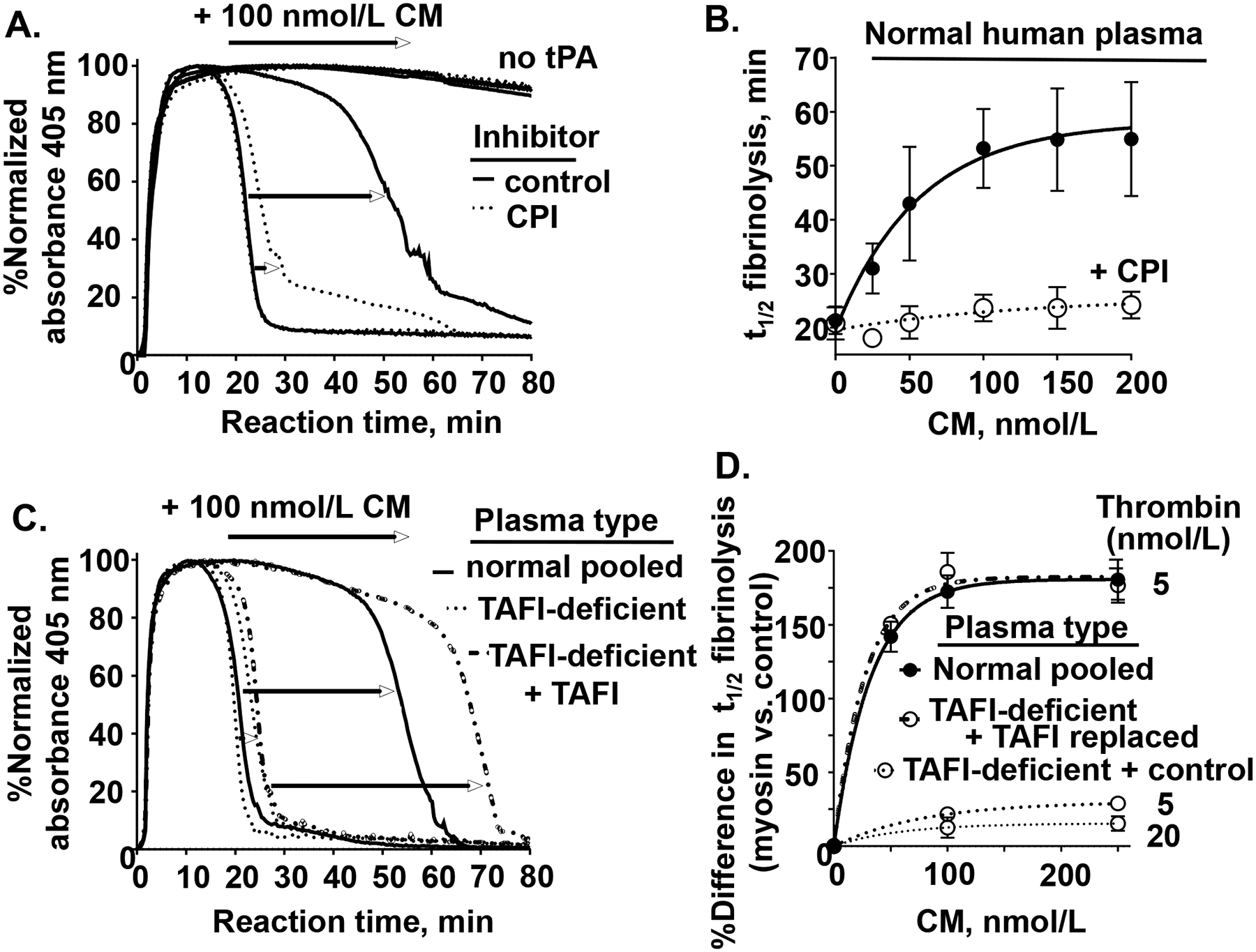
Objective: Cardiac myosin (CM) is structurally similar to skeletal muscle myosin, which has procoagulant activity. Here, we evaluated CM's ex vivo, in vivo, and in vitro activities related to hemostasis and thrombosis. Approach and Results: Perfusion of fresh human blood over CM-coated surfaces caused thrombus formation and fibrin deposition. Addition of CM to blood passing over collagen-coated surfaces enhanced fibrin formation. In a murine ischemia/reperfusion injury model, exogenous CM, when administered intravenously, augmented myocardial infarction and troponin I release. In hemophilia A mice, intravenously administered CM reduced tail-cut-initiated bleeding. These data provide proof of concept for CM's in vivo procoagulant properties. In vitro studies clarified some mechanisms for CM's procoagulant properties. Thrombin generation assays showed that CM, like skeletal muscle myosin, enhanced thrombin generation in human platelet-rich and platelet-poor plasmas and also in mixtures of purified factors Xa, Va, and prothrombin. Binding studies showed that CM, like skeletal muscle myosin, directly binds factor Xa, supporting the concept that the CM surface is a site for prothrombinase assembly. In tPA (tissue-type plasminogen activator)-induced plasma clot lysis assays, CM was antifibrinolytic due to robust CM-dependent thrombin generation that enhanced activation of TAFI (thrombin activatable fibrinolysis inhibitor).
Conclusions: CM in vitro is procoagulant and prothrombotic. CM in vivo can augment myocardial damage and can be prohemostatic in the presence of bleeding. CM's procoagulant and antifibrinolytic activities likely involve, at least in part, its ability to bind factor Xa and enhance thrombin generation. Future work is needed to clarify CM's pathophysiology and its mechanistic influences on hemostasis or thrombosis.
Keywords: cardiac myosins; fibrin; hemostasis; thrombin; thrombosis.
Conflict of interest statement
Figures
References
-
- Fuster V, Badimon L, Cohen M, Ambrose JA, Badimon JJ and Chesebro J. Insights into the pathogenesis of acute ischemic syndromes. Circulation. 1988;77:1213–1220. - PubMed
-
- Herrick JB. Landmark article (JAMA 1912). Clinical features of sudden obstruction of the coronary arteries. By James B. Herrick. Jama. 1983;250:1757–1765. - PubMed
-
- Gorlin R, Fuster V and Ambrose JA. Anatomic-physiologic links between acute coronary syndromes. Circulation. 1986;74:6–9. - PubMed
-
- Baumgartner HR. New aspects in thrombogenesis. VASA Zeitschrift fur Gefasskrankheiten. 1974;3:60–64. - PubMed
-
- Khaw BA, Gold HK, Fallon JT and Haber E. Detection of serum cardiac myosin light chains in acute experimental myocardial infarction: radioimmunoassay of cardiac myosin light chains. Circulation. 1978;58:1130–1136. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
