

Estimating the burden of iron deficiency among African children
- PMID: 32102669
- PMCID: PMC7045745
- DOI: 10.1186/s12916-020-1502-7
Estimating the burden of iron deficiency among African children
Abstract
Background: Iron deficiency (ID) is a major public health burden in African children and accurate prevalence estimates are important for effective nutritional interventions. However, ID may be incorrectly estimated in Africa because most measures of iron status are altered by inflammation and infections such as malaria. Through the current study, we have assessed different approaches to the prediction of iron status and estimated the burden of ID in African children.
Methods: We assayed iron and inflammatory biomarkers in 4853 children aged 0-8 years from Kenya, Uganda, Burkina Faso, South Africa, and The Gambia. We described iron status and its relationship with age, sex, inflammation, and malaria parasitemia. We defined ID using the WHO guideline (ferritin < 12 μg/L or < 30 μg/L in the presence of inflammation in children < 5 years old or < 15 μg/L in children ≥ 5 years old). We compared this with a recently proposed gold standard, which uses regression-correction for ferritin levels based on the relationship between ferritin levels, inflammatory markers, and malaria. We further investigated the utility of other iron biomarkers in predicting ID using the inflammation and malaria regression-corrected estimate as a gold standard.
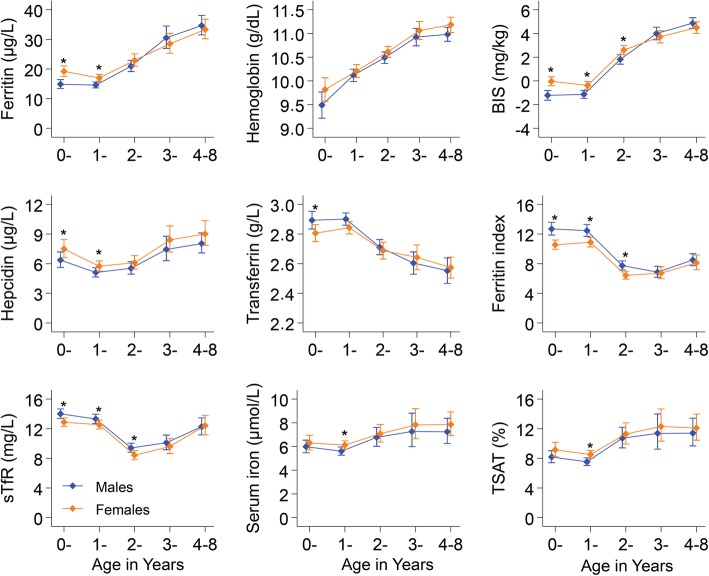
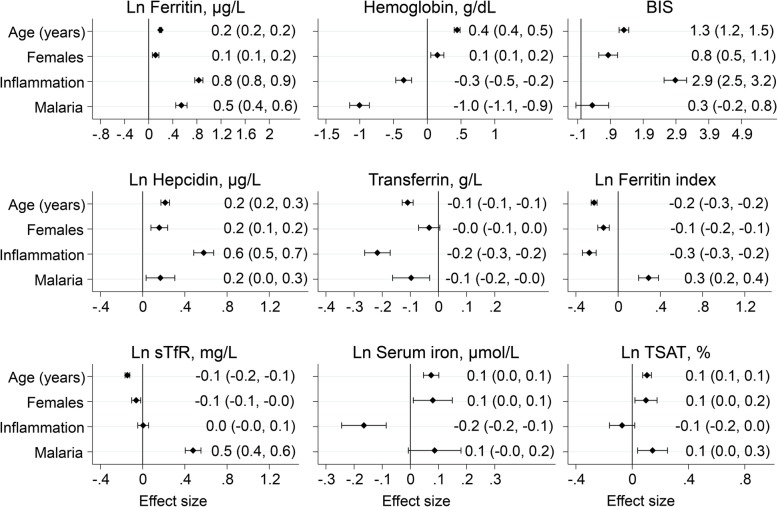
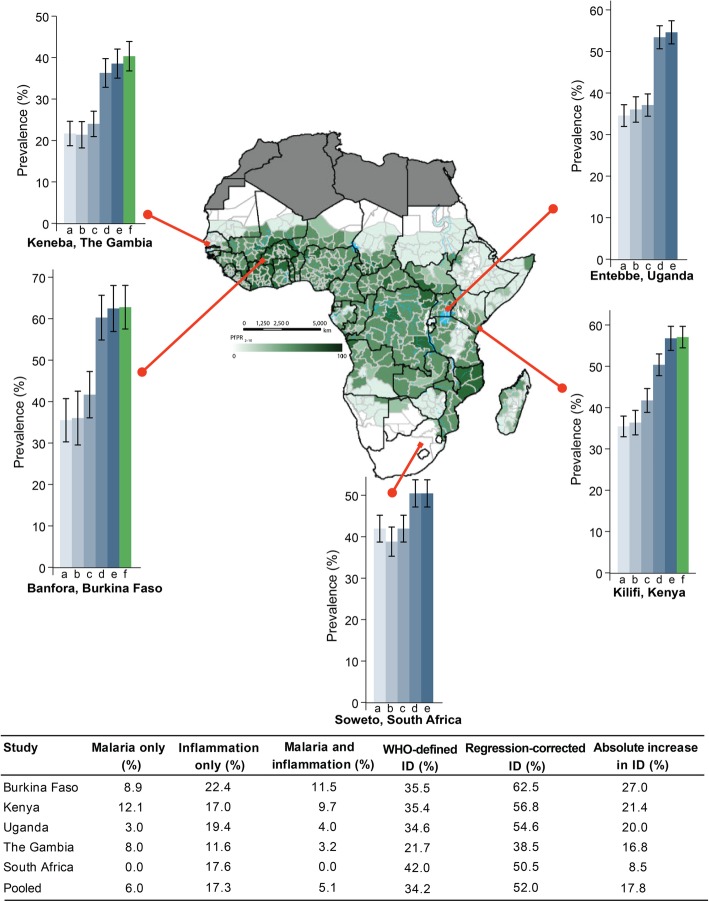
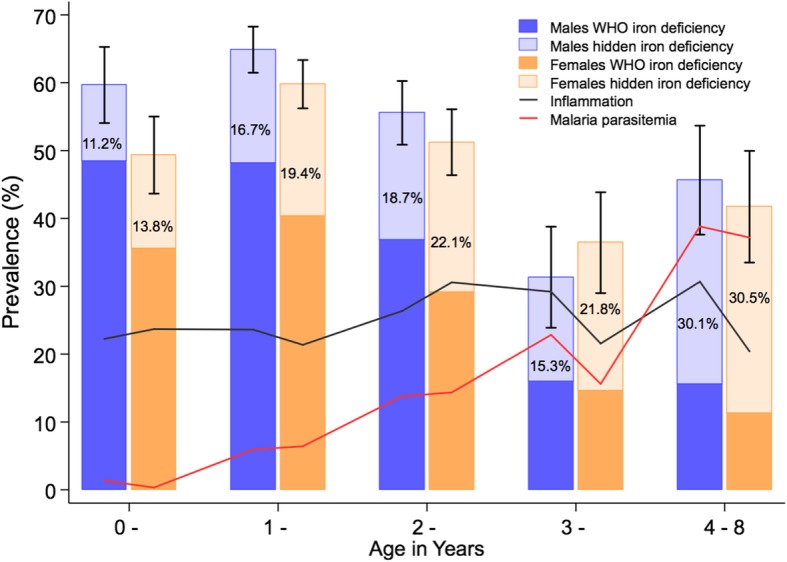
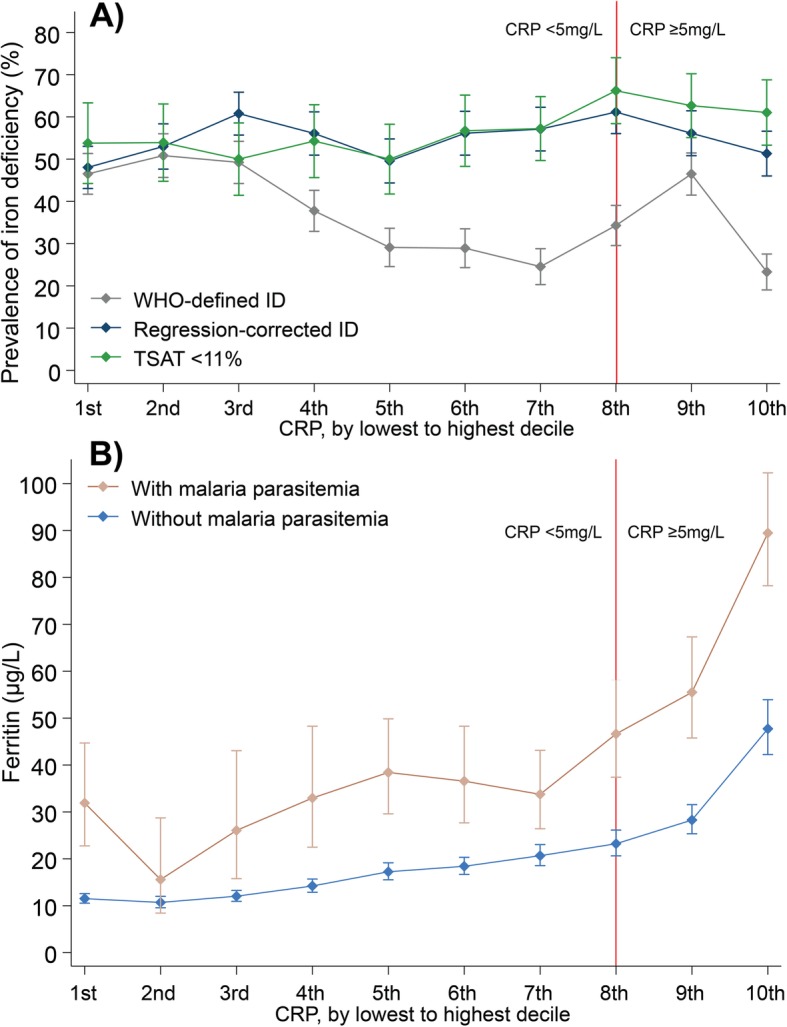
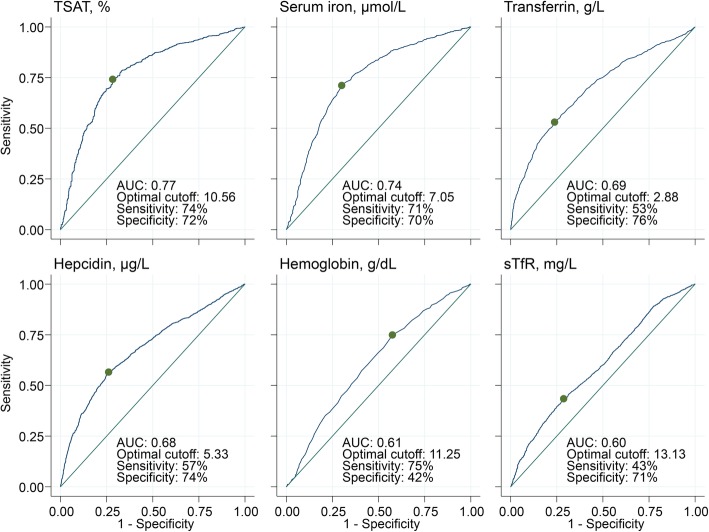
Results: The prevalence of ID was highest at 1 year of age and in male infants. Inflammation and malaria parasitemia were associated with all iron biomarkers, although transferrin saturation was least affected. Overall prevalence of WHO-defined ID was 34% compared to 52% using the inflammation and malaria regression-corrected estimate. This unidentified burden of ID increased with age and was highest in countries with high prevalence of inflammation and malaria, where up to a quarter of iron-deficient children were misclassified as iron replete. Transferrin saturation < 11% most closely predicted the prevalence of ID according to the regression-correction gold standard.
Conclusions: The prevalence of ID is underestimated in African children when defined using the WHO guidelines, especially in malaria-endemic populations, and the use of transferrin saturation may provide a more accurate approach. Further research is needed to identify the most accurate measures for determining the prevalence of ID in sub-Saharan Africa.
Keywords: African children; Ferritin; Inflammation; Iron deficiency; Malaria; Transferrin saturation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- GBD-2016-Disease-and-Injury-Incidence-and-Prevalence-Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211–1259. doi: 10.1016/S0140-6736(17)32154-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- MC_UU_00027/5/MRC_/Medical Research Council/United Kingdom
- 202800/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- EP-C-15-003/EPA/EPA/United States
- 064693/WT_/Wellcome Trust/United Kingdom
- MC_PC_MR/R020183/1/MRC_/Medical Research Council/United Kingdom
- MR/R010161/1/MRC_/Medical Research Council/United Kingdom
- 203077/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- MC_U123292699/MRC_/Medical Research Council/United Kingdom
- MC_UU_00026/3/MRC_/Medical Research Council/United Kingdom
- 106289/Z/14/Z/WT_/Wellcome Trust/United Kingdom
- 095778/WT_/Wellcome Trust/United Kingdom
- MC-A760-5QX00/Bill and Melinda Gates Foundation/International
- 110255/Z/15/Z/WT_/Wellcome Trust/United Kingdom
- 079110/WT_/Wellcome Trust/United Kingdom
- 294557/FP7 Ideas: European Research Council/International
LinkOut - more resources
Full Text Sources
