

Neuropsychological and neuroanatomical phenotype in 17 patients with cystinosis
- PMID: 32102670
- PMCID: PMC7045592
- DOI: 10.1186/s13023-019-1271-6
Neuropsychological and neuroanatomical phenotype in 17 patients with cystinosis
Abstract
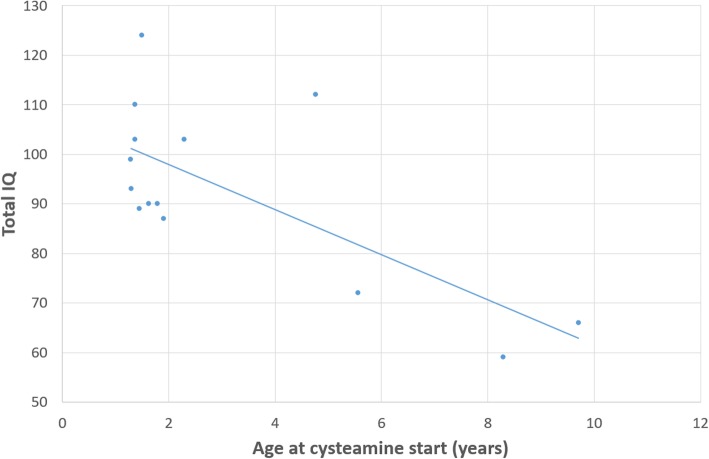
Background: Cystinosis is a rare autosomal recessive disorder caused by intracellular cystine accumulation. Proximal tubulopathy (Fanconi syndrome) is one of the first signs, leading to end-stage renal disease between the age of 12 and 16. Other symptoms occur later and encompass endocrinopathies, distal myopathy and deterioration of the central nervous system. Treatment with cysteamine if started early can delay the progression of the disease. Little is known about the neurological impairment which occurs later. The goal of the present study was to find a possible neuroanatomical dysmorphic pattern that could help to explain the cognitive profile of cystinosis patients. We also performed a detailed review of the literature on neurocognitive complications associated with cystinosis.
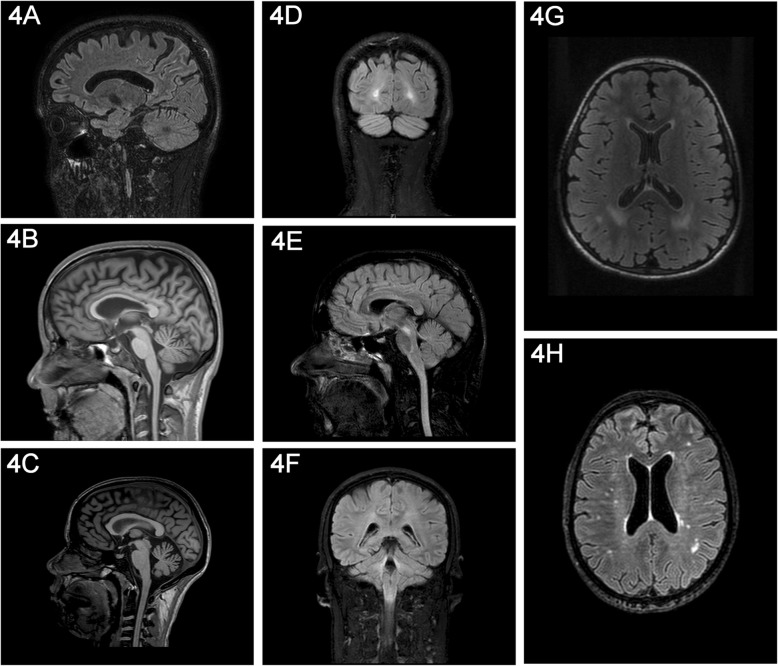
Methods: 17 patients (mean age = 17.6 years, [5.4-33.3]) with cystinosis were included in the study. Neuropsychological assessment was performed including intelligence (Intelligence Quotient (IQ) with Wechsler's scale), memory (Children Memory Scale and Wechsler Memory Scale), visuo-spatial (Rey's figure test) and visuo-perceptual skills assessments. Structural brain MRI (3 T) was also performed in 16 out of 17 patients, with high resolution 3D T1-weighted, 3D FLAIR and spectroscopy sequences.
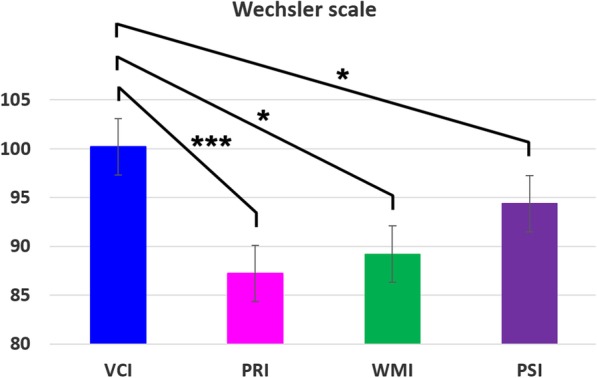
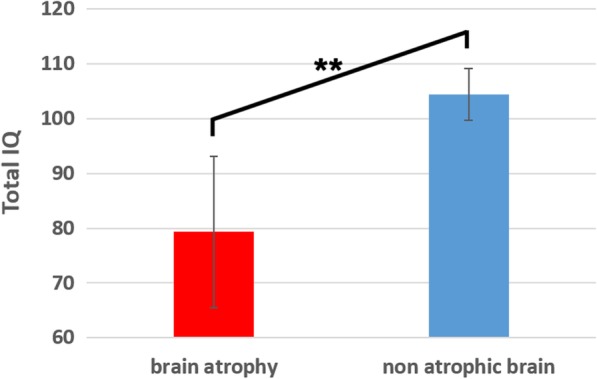
Results: Intellectual efficiency was normal in patients with cystinosis (mean Total IQ = 93). However the Perceptual Reasoning Index (mean = 87, [63-109]) was significantly lower than the Verbal Comprehension Index (mean = 100, [59-138], p = 0.003). Memory assessment showed no difference between visual and verbal memory. But the working memory was significantly impaired in comparison with the general memory skills (p = 0.003). Visuospatial skills assessment revealed copy and reproduction scores below the 50th percentile rank in more than 70% of the patients. Brain MRI showed cortical and sub-cortical cerebral atrophy, especially in the parieto-occipital region and FLAIR hypersignals in parietal, occipital and brain stem/cerebellum. Patients with atrophic brain had lower Total IQ scores compared to non-atrophic cystinosis patients.
Conclusions: Patients with cystinosis have a specific neuropsychological and neuroanatomical profile. We suggest performing a systematic neuropsychological assessment in such children aiming at considering adequate management.
Keywords: Cystinosis; Neuroimaging; Neuropsychological profile.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Emma F, Nesterova G, Langman C, Labbe A, Cherqui S, Goodyer P, Janssen MC, Greco M, Topaloglu R, Elenberg E, Dohil R, Trauner D, Antignac C, Cochat P, Kaskel F, Servais A, Wuhl E, Niaudet P, Van't Hoff W, Gahl W, Levtchenko E. Nephropathic cystinosis: an international consensus document. Nephrol Dial Transplant. 2014;29(Suppl 4):iv87–iv94. doi: 10.1093/ndt/gfu090. - DOI - PMC - PubMed
-
- Broyer M, Guillot M, Gubler MC, Habib R. Infantile cystinosis: a reappraisal of early and late symptoms. Adv Nephrol Necker Hosp. 1981;10:137–166. - PubMed
-
- Brodin-Sartorius A, Tete MJ, Niaudet P, Antignac C, Guest G, Ottolenghi C, Charbit M, Moyse D, Legendre C, Lesavre P, Cochat P, Servais A. Cysteamine therapy delays the progression of nephropathic cystinosis in late adolescents and adults. Kidney Int. 2012;81(2):179–189. doi: 10.1038/ki.2011.277. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
