

Comparison of T-piece and pressure support ventilation as spontaneous breathing trials in critically ill patients: a systematic review and meta-analysis
- PMID: 32102693
- PMCID: PMC7045460
- DOI: 10.1186/s13054-020-2764-3
Comparison of T-piece and pressure support ventilation as spontaneous breathing trials in critically ill patients: a systematic review and meta-analysis
Abstract
Background: The effect of alternative spontaneous breathing trial (SBT) techniques on extubation success and other clinically important outcomes is uncertain. A systematic review and meta-analysis was performed to clarify the preferable SBT (T-piece or pressure support ventilation [PSV]).
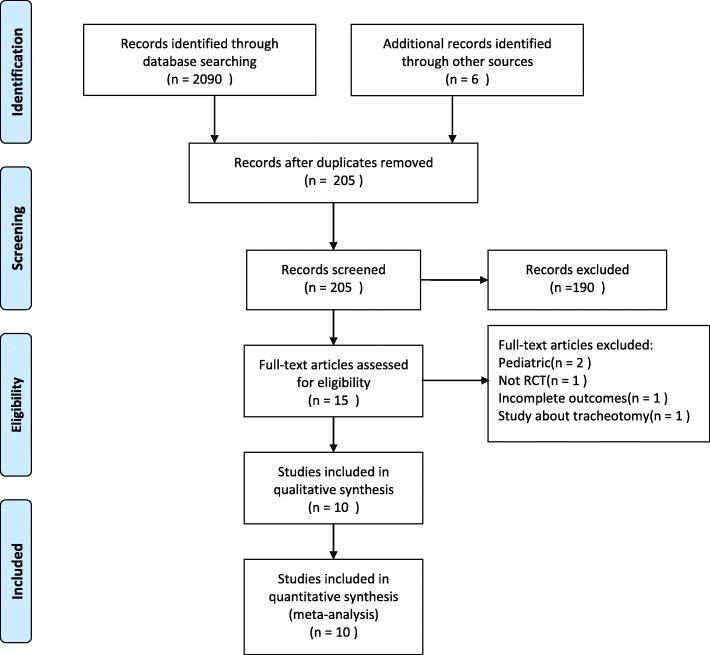
Methods: We searched the PubMed, Cochrane, and Embase databases for randomized controlled trials (RCTs) from inception to the 31st of July 2019. We included RCTs involving adult patients (> 18 years) who underwent at least two different SBT methods. All authors reported our primary outcome of successful extubation rate and clearly compared PS versus T-piece with clinically relevant secondary outcomes (rate of reintubation, ICU and hospital length of stay, and ICU and hospital mortality). Results were expressed as odds ratio (OR) and mean difference (MD) with accompanying 95% confidence interval (CI).
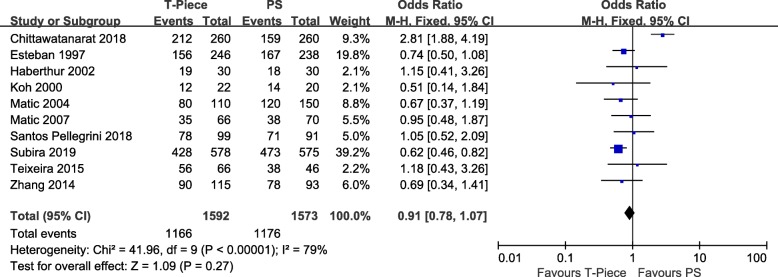
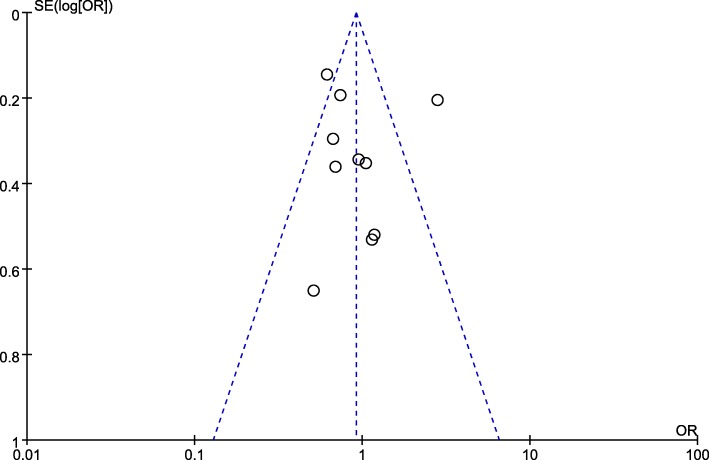
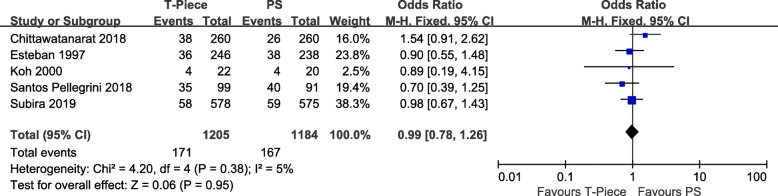
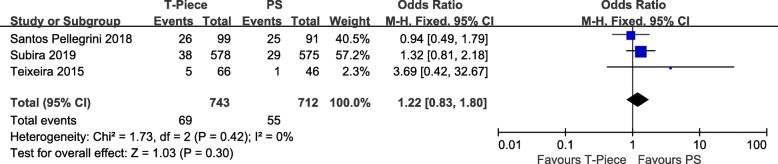
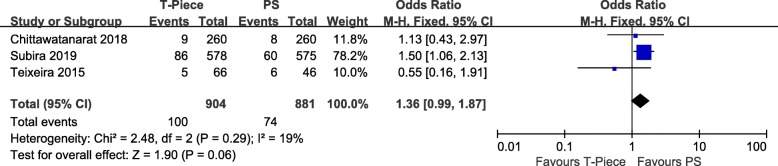
Results: Ten RCTs including 3165 patients were included. The results of this meta-analysis showed that there was no significant difference in the successful extubation rate between the T-piece group and PS group (odds ratio [OR] = 0.91; 95% CI, 0.78-1.07; P = 0.27; I2 = 79%). In addition, compared with the PS group, the T-piece group showed no significant difference in the rate of reintubation (odds ratio [OR] = 0.99; 95% CI, 0.78-1.26; P = 0.95; I2 = 5%), ICU mortality (odds ratio [OR] = 1.22; 95% CI, 0.83-1.80; P = 0.30; I2 = 0%), hospital mortality (odds ratio [OR] = 1.36; 95% CI, 0.99-1.87; P = 0.06; I2 = 19%), ICU length of stay (mean difference = - 0.10; 95% CI, - 0.59 to 0.39; P = 0.69; I2 = 13%), and hospital length of stay (mean difference = - 0.82;95% CI, - 2.2 to 0.55; P = 0.24; I2 = 0%).
Conclusions: T-piece and PSV as SBTs are considered to have comparable predictive power of successful extubation in critically ill patients. The analysis of secondary outcomes also shows no significant difference in the rate of reintubation, ICU and hospital length of stay, and ICU and hospital mortality between the two groups. Further randomized controlled studies of SBTs are still required.
Keywords: Meta-analysis; Pressure support ventilation; Randomized controlled trials; Spontaneous breathing trials; Systematic review; T-piece.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Sklar MC, Burns K, Rittayamai N, Lanys A, Rauseo M, Chen L, Dres M, Chen GQ, Goligher EC, Adhikari NKJ, Brochard, et al. Effort to breathe with various spontaneous breathing trial techniques. A physiologic meta-analysis. Am J Respir Crit Care Med. 2017;195(11):1477–1485. doi: 10.1164/rccm.201607-1338OC. - DOI - PubMed
-
- Esteban A, Anzueto A, Frutos F, Alía I, Brochard L, Stewart TE, Benito S, Epstein SK, Apezteguía C, Nightingale P, et al. Mechanical Ventilation International Study Group. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA. 2002;287(3):345–355. doi: 10.1001/jama.287.3.345. - DOI - PubMed
-
- Peñuelas O, Frutos-Vivar F, Fernández C, Anzueto A, Epstein SK, Apezteguía C, González M, Nin N, Raymondos K, Tomicic V, et al. Characteristics and outcomes of ventilated patients according to time to liberation from mechanical ventilation. Am J Respir Crit Care Med. 2011;184(4):430–437. doi: 10.1164/rccm.201011-1887OC. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
