

Albumin in decompensated cirrhosis: new concepts and perspectives
- PMID: 32102926
- PMCID: PMC7282556
- DOI: 10.1136/gutjnl-2019-318843
Albumin in decompensated cirrhosis: new concepts and perspectives
Abstract
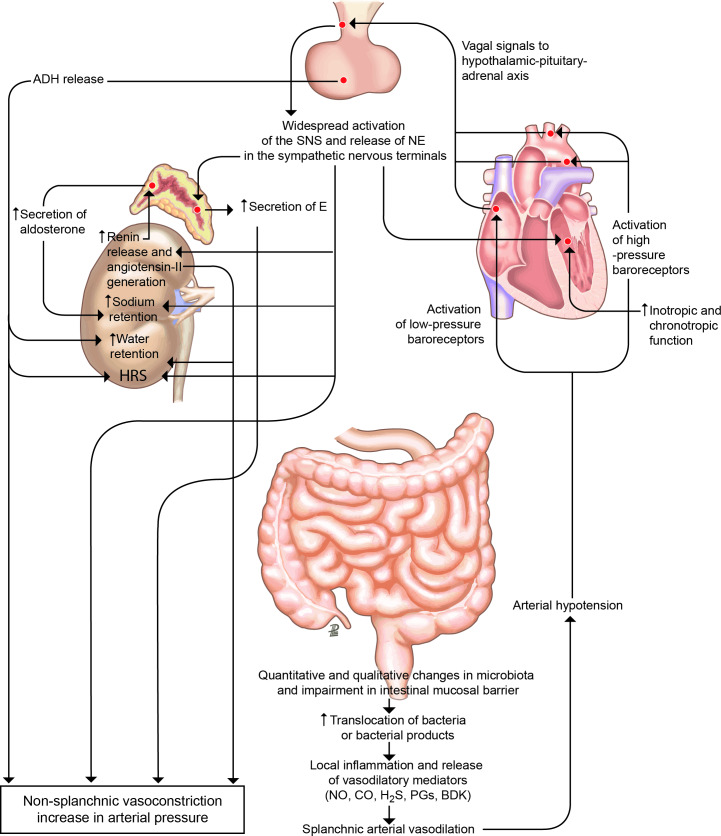
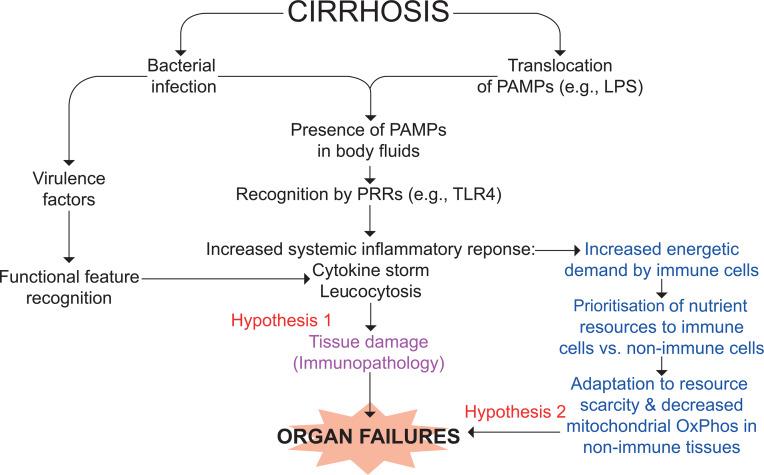
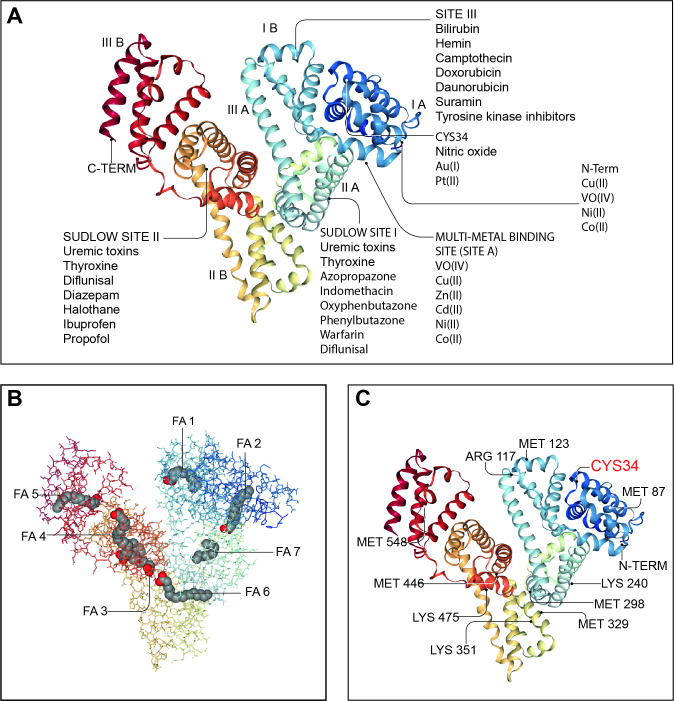
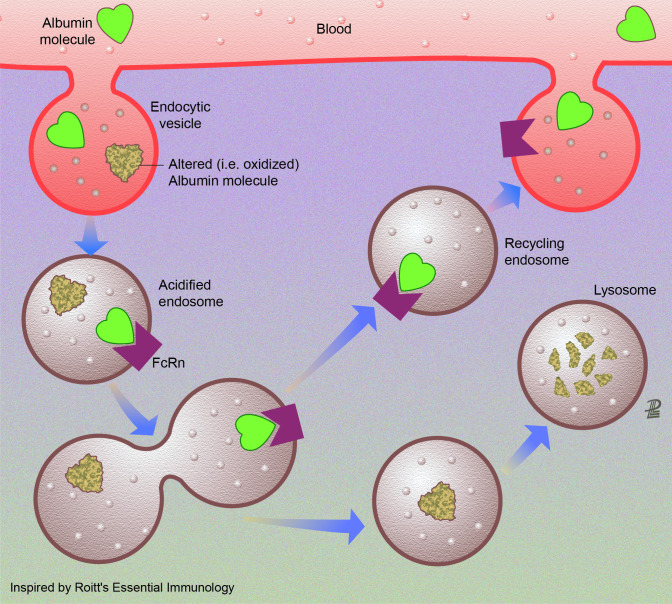
The pathophysiological background of decompensated cirrhosis is characterised by a systemic proinflammatory and pro-oxidant milieu that plays a major role in the development of multiorgan dysfunction. Such abnormality is mainly due to the systemic spread of bacteria and/or bacterial products from the gut and danger-associated molecular patterns from the diseased liver triggering the release of proinflammatory mediators by activating immune cells. The exacerbation of these processes underlies the development of acute-on-chronic liver failure. A further mechanism promoting multiorgan dysfunction and failure likely consists with a mitochondrial oxidative phosphorylation dysfunction responsible for systemic cellular energy crisis. The systemic proinflammatory and pro-oxidant state of patients with decompensated cirrhosis is also responsible for structural and functional changes in the albumin molecule, which spoil its pleiotropic non-oncotic properties such as antioxidant, scavenging, immune-modulating and endothelium protective functions. The knowledge of these abnormalities provides novel targets for mechanistic treatments. In this respect, the oncotic and non-oncotic properties of albumin make it a potential multitarget agent. This would expand the well-established indications to the use of albumin in decompensated cirrhosis, which mainly aim at improving effective volaemia or preventing its deterioration. Evidence has been recently provided that long-term albumin administration to patients with cirrhosis and ascites improves survival, prevents complications, eases the management of ascites and reduces hospitalisations. However, variant results indicate that further investigations are needed, aiming at confirming the beneficial effects of albumin, clarifying its optimal dosage and administration schedule and identify patients who would benefit most from long-term albumin administration.
Keywords: liver cirrhosis.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: PG is recipient of an ICREA Academia Award. MB: personal fees from CLS Behring GmbH, personal fees from Grifols SA, personal fees from Takeda, personal fees from Martin Pharmaceuticals, personal fees from PPTA, personal fees from Octapharma, outside the submitted work. PA: personal fees from Grifols, grants from CLS Behring, outside the submitted work. PG: grants and personal fees from GILEAD, grants and personal fees from Mallinckrodt, grants and personal fees from Grifols, personal fees from Intercept, personal fees from Martin Phamaceuticals, personal fees from Sequana, personal fees from Promethera, outside the submitted work. RJ: other from Yaqrit Limited, grants from Takeda, other from Kaleido, from Akaza, from Mallinkrodt, other from Prometic, grants and other from Theoris, during the conduct of the study; other from Yaqrit Limited, grants from Takeda, other from Kaleido, other from Akaza, other from Prometic, other from Mallinkrodt, grants and other from Theoris, outside the submitted work. PC: personal fees from Grifols SA, grants and personal fees from Octapharma SA, personal fees from Kedrion SpA, personal fees from Takeda SA, personal fees from Alphasigma SA, outside the submitted work. JF: personal fees and other from Grifols, outside the submitted work. ALG: personal fees from CLS Behring, personal fees from Grifols, outside the submitted work. JT: personal fees from Gore, personal fees from Bayer, personal fees from Alexion, personal fees from MSD, personal fees from Gilead, personal fees from Intercept, personal fees from Norgine, personal fees from Grifols, personal fees from Versantis, personal fees from Martin Pharmaceutical outside submitted work. VA: personal fees from Grifols, outside the submitted work; VA has a patent 'method for diagnostic and/or prognostic of acute on-chronic liver failure syndrome in patients with liver disorders' pending.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical