

Baseline Plasma Tumor Mutation Burden Predicts Response to Pembrolizumab-based Therapy in Patients with Metastatic Non-Small Cell Lung Cancer
- PMID: 32102950
- PMCID: PMC7231655
- DOI: 10.1158/1078-0432.CCR-19-3663
Baseline Plasma Tumor Mutation Burden Predicts Response to Pembrolizumab-based Therapy in Patients with Metastatic Non-Small Cell Lung Cancer
Abstract
Purpose: The role of plasma-based tumor mutation burden (pTMB) in predicting response to pembrolizumab-based first-line standard-of-care therapy for metastatic non-small cell lung cancer (mNSCLC) has not been explored.
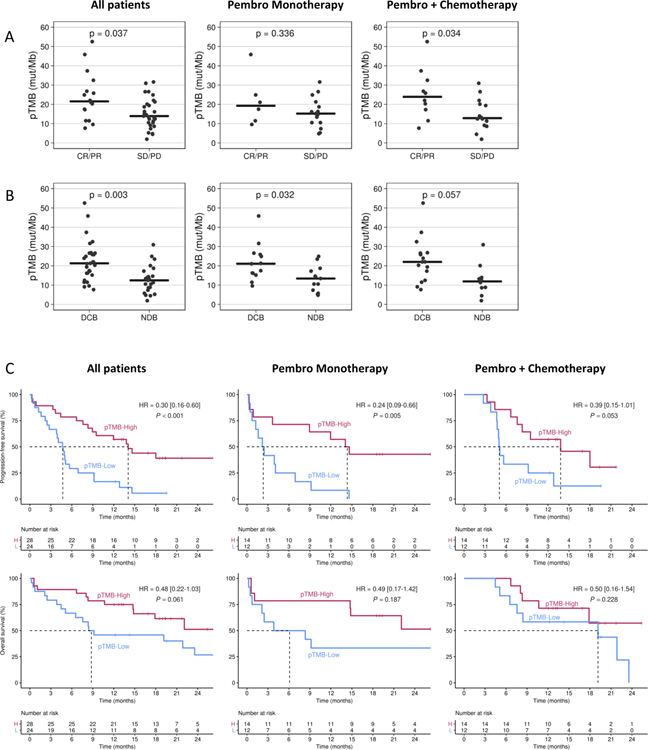
Experimental design: A 500-gene next-generation sequencing panel was used to assess pTMB. Sixty-six patients with newly diagnosed mNSCLC starting first-line pembrolizumab-based therapy, either alone or in combination with chemotherapy, were enrolled (Clinicaltrial.gov identifier: NCT03047616). Response was assessed using RECIST 1.1. Associations were made for patient characteristics, 6-month durable clinical benefit (DCB), progression-free survival (PFS), and overall survival (OS).
Results: Of 66 patients, 52 (78.8%) were pTMB-evaluable. Median pTMB was 16.8 mutations per megabase (mut/Mb; range, 1.9-52.5) and was significantly higher for patients achieving DCB compared with no durable benefit (21.3 mut/Mb vs. 12.4 mut/Mb, P = 0.003). For patients with pTMB ≥ 16 mut/Mb, median PFS was 14.1 versus 4.7 months for patients with pTMB < 16 mut/Mb [HR, 0.30 (0.16-0.60); P < 0.001]. Median OS for patients with pTMB ≥ 16 was not reached versus 8.8 months for patients with pTMB < 16 mut/Mb [HR, 0.48 (0.22-1.03); P = 0.061]. Mutations in ERBB2 exon 20, STK11, KEAP1, or PTEN were more common in patients with no DCB. A combination of pTMB ≥ 16 and absence of negative predictor mutations was associated with PFS [HR, 0.24 (0.11-0.49); P < 0.001] and OS [HR, 0.31 (0.13-0.74); P = 0.009].
Conclusions: pTMB ≥ 16 mut/Mb is associated with improved PFS after first-line standard-of-care pembrolizumab-based therapy in mNSCLC. STK11/KEAP1/PTEN and ERBB2 mutations may help identify pTMB-high patients unlikely to respond. These results should be validated in larger prospective studies.
©2020 American Association for Cancer Research.
Conflict of interest statement
Disclosures:
The authors have declared no conflicts of interest.
Figures

Comment in
-
Plasma Tumor Mutation Burden and Response to Pembrolizumab-Letter.Clin Cancer Res. 2020 Jul 1;26(13):3491. doi: 10.1158/1078-0432.CCR-20-0903. Clin Cancer Res. 2020. PMID: 32611625 No abstract available.
-
Plasma Tumor Mutation Burden and Response to Pembrolizumab-Response.Clin Cancer Res. 2020 Jul 1;26(13):3492. doi: 10.1158/1078-0432.CCR-20-1073. Clin Cancer Res. 2020. PMID: 32611626 Free PMC article. No abstract available.
-
Plasma Tumor Mutation Burden and Response to Pembrolizumab-Letter.Clin Cancer Res. 2021 Mar 1;27(5):1580. doi: 10.1158/1078-0432.CCR-20-2698. Clin Cancer Res. 2021. PMID: 33649190 No abstract available.
-
Plasma Tumor Mutation Burden and Response to Pembrolizumab-Response.Clin Cancer Res. 2021 Mar 1;27(5):1581. doi: 10.1158/1078-0432.CCR-20-4753. Clin Cancer Res. 2021. PMID: 33649191 No abstract available.
References
-
- Reck M, et al., Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med, 2016. 375(19): p. 1823–1833. - PubMed
-
- Gandhi L, et al., Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N Engl J Med, 2018. 378(22): p. 2078–2092. - PubMed
-
- Paz-Ares L, et al., Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N Engl J Med, 2018. 379(21): p. 2040–2051. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
