

Prevalence of Self-reported Neurologic and Ocular Symptoms in Early Syphilis Cases
- PMID: 32103243
- PMCID: PMC11310899
- DOI: 10.1093/cid/ciaa180
Prevalence of Self-reported Neurologic and Ocular Symptoms in Early Syphilis Cases
Abstract
Background: Neurosyphilis, a complication of syphilis, can occur at any stage of infection. Measuring the prevalence of neurosyphilis is challenging, and there are limited data on the prevalence of neurologic or ocular symptoms among patients with syphilis. We sought to describe the prevalence of neurologic and/or ocular symptoms among early syphilis (ES) cases and the clinical management of symptomatic cases enrolled in the STD Surveillance Network (SSuN) Neuro/Ocular Syphilis Surveillance project.
Methods: Persons diagnosed with ES were selected for interviews based on current health department protocols in 5 participating SSuN jurisdictions from November 2016 through October 2017. All interviewed ES cases were screened for self-reported neurologic and/or ocular symptoms. Additional clinical information on diagnostic testing and treatment for cases concerning for neurosyphilis/ocular syphilis was obtained from providers.
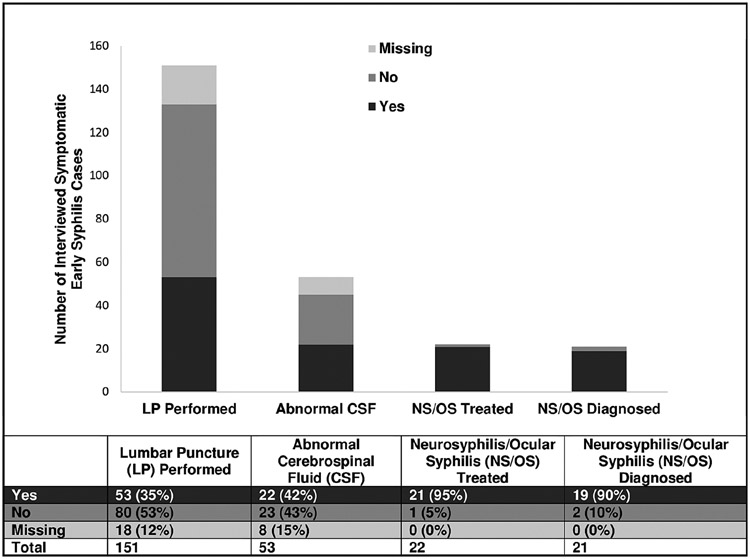
Results: Among 9123 patients with ES who were interviewed, 151 (1.7%; 95% confidence interval [CI], 1.4%-1.9%) reported ≥ 1 neurologic or ocular symptom. Of the 53 (35%) who underwent lumbar puncture, 22 (42%) had documented abnormal cerebrospinal fluid, of which 21 (95%) were treated for neurosyphilis/ocular syphilis. Among the remaining 98 symptomatic patients with no documented lumbar puncture (65%), 12 (12%) were treated for and/or clinically diagnosed with neurosyphilis/ocular syphilis.
Conclusions: We observed a low prevalence of self-reported neurologic and/or ocular symptoms in interviewed ES cases. Approximately one-third of ES cases who self-reported symptoms underwent further recommended diagnostic evaluation. Understanding barriers to appropriate clinical evaluation is important to ensuring appropriate management of patients with possible neurologic and/or ocular manifestations of syphilis.
Keywords: complicated syphilis; early syphilis; neurosyphilis; ocular syphilis; prevalence.
Published by Oxford University Press for the Infectious Diseases Society of America 2020.
Conflict of interest statement
Figures
References
-
- Lukehart SA, Hook EW 3rd, Baker-Zander SA, Collier AC, Critchlow CW, Handsfield HH. Invasion of the central nervous system by Treponema pallidum: implications for diagnosis and treatment. Ann Intern Med 1988; 109:855–62. - PubMed
-
- Rolfs RT, Joesoef MR, Hendershot EF, et al. A randomized trial of enhanced therapy for early syphilis in patients with and without human immunodeficiency virus infection. The Syphilis and HIV Study Group. N Engl J Med 1997; 337:307–14. - PubMed
-
- Merritt HH, Adams AR, Solomon HC. Neurosyphilis. New York: Oxford, 1946.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
