

Alternative Lengthening of Telomeres and Differential Expression of Endocrine Transcription Factors Distinguish Metastatic and Non-metastatic Insulinomas
- PMID: 32103422
- PMCID: PMC7250793
- DOI: 10.1007/s12022-020-09611-8
Alternative Lengthening of Telomeres and Differential Expression of Endocrine Transcription Factors Distinguish Metastatic and Non-metastatic Insulinomas
Abstract
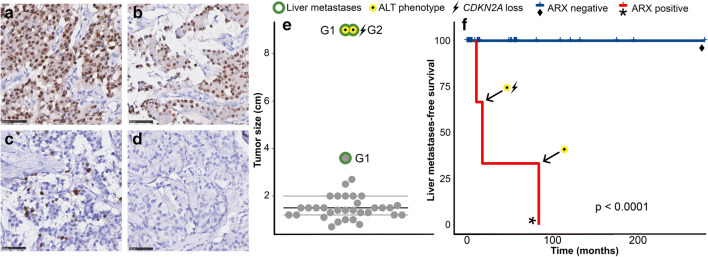
Insulin-producing pancreatic neuroendocrine tumors (PanNETs)/insulinomas are generally considered to be indolent tumors with an excellent prognosis after complete resection. However, some insulinomas have a poor prognosis due to relapses and metastatic disease. Recently, studies in non-functional PanNETs indicated that behavior can be stratified according to alpha- and beta-cell differentiation, as defined by expression of the transcription factors ARX and PDX1, respectively. It is unknown whether similar mechanisms play a role in insulinomas. Therefore, we determined ARX and PDX1 expression in a cohort of 35 sporadic primary insulinomas and two liver metastases of inoperable primary insulinomas. In addition, WHO grade and loss of ATRX or DAXX were determined by immunohistochemistry, and alternative lengthening of telomeres (ALT) and CDKN2A status by fluorescence in situ hybridization. These findings were correlated with tumor characteristics and clinical follow-up data. In total, five out of 37 insulinoma patients developed metastatic disease. Metastatic insulinomas were all larger than 3 cm, whereas the indolent insulinomas were smaller (p value < 0.05). All three primary insulinomas that metastasized showed ARX expression, 2/3 showed ALT, and 1/3 had a homozygous deletion of CDKN2A as opposed to absence of ARX expression, ALT, or CDKN2A deletions in the 32 non-metastatic cases. The two liver metastases also showed ARX expression and ALT (2/2). The presence of ARX expression, which is usually absent in beta-cells, and genetic alterations not seen in indolent insulinomas strongly suggest a distinct tumorigenic mechanism in malignant insulinomas, with similarities to non-functional PanNETs. These observations may inform future follow-up strategies after insulinoma surgery.
Keywords: Insulinoma; Liver metastasis; Malignant insulinoma; Neuroendocrine cells; Pancreatic neuroendocrine tumor.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Camara-de-Souza AB, Toyoshima MTK, Giannella ML, Freire DS, Camacho CP, Lourenco DM, Jr, Rocha MS, Bacchella T, Jureidini R, Machado MCC, Almeida MQ, Pereira MAA. Insulinoma: A retrospective study analyzing the differences between benign and malignant tumors. Pancreatology. 2018;18(3):298–303. doi: 10.1016/j.pan.2018.01.009. - DOI - PubMed
-
- Nikfarjam M, Warshaw AL, Axelrod L, Deshpande V, Thayer SP, Ferrone CR, Fernandez-del Castillo C. Improved contemporary surgical management of insulinomas: a 25-year experience at the Massachusetts General Hospital. Ann Surg. 2008;247(1):165–172. doi: 10.1097/SLA.0b013e31815792ed. - DOI - PMC - PubMed
-
- Falconi M, Eriksson B, Kaltsas G, Bartsch DK, Capdevila J, Caplin M, Kos-Kudla B, Kwekkeboom D, Rindi G, Kloppel G, Reed N, Kianmanesh R, Jensen RT, Vienna Consensus Conference p ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology. 2016;103(2):153–171. doi: 10.1159/000443171. - DOI - PMC - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
