

Evaluation of the clinical impact of repeat application of hydrogel-forming microneedle array patches
- PMID: 32103450
- PMCID: PMC7228965
- DOI: 10.1007/s13346-020-00727-2
Evaluation of the clinical impact of repeat application of hydrogel-forming microneedle array patches
Abstract
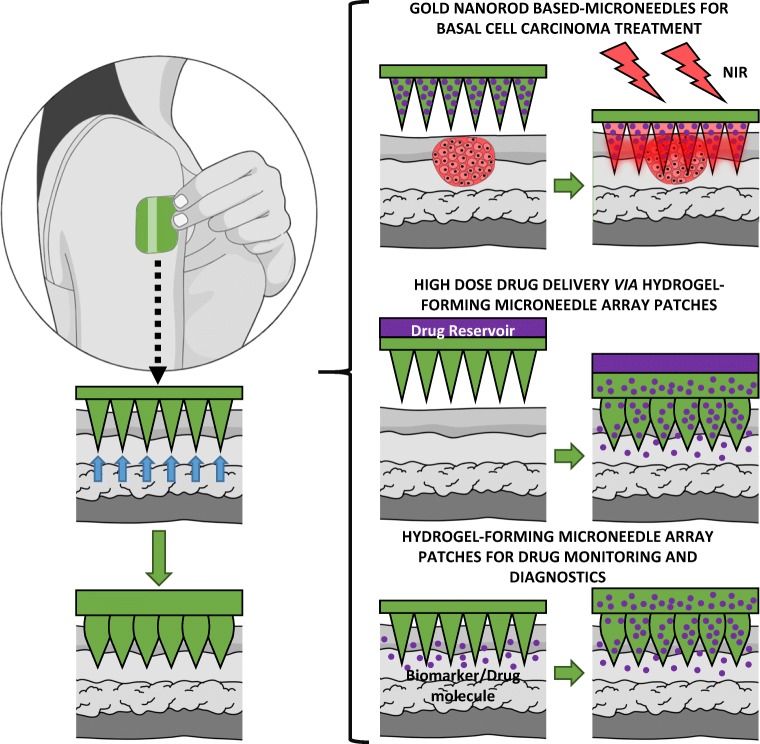
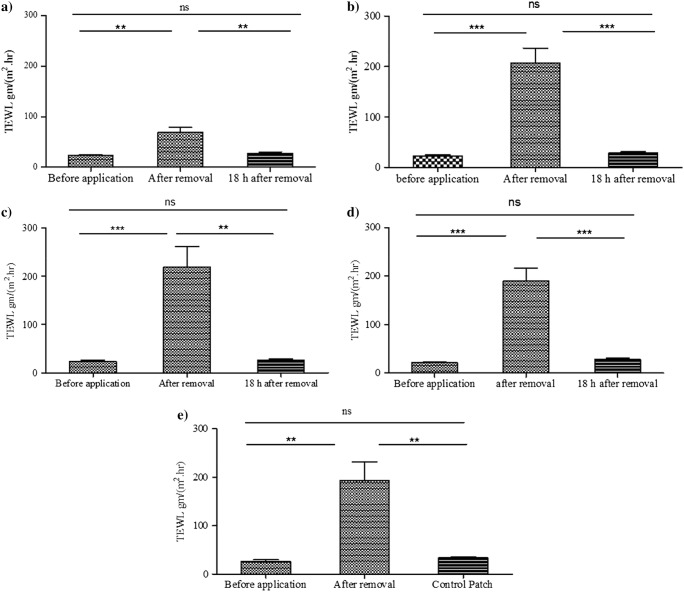
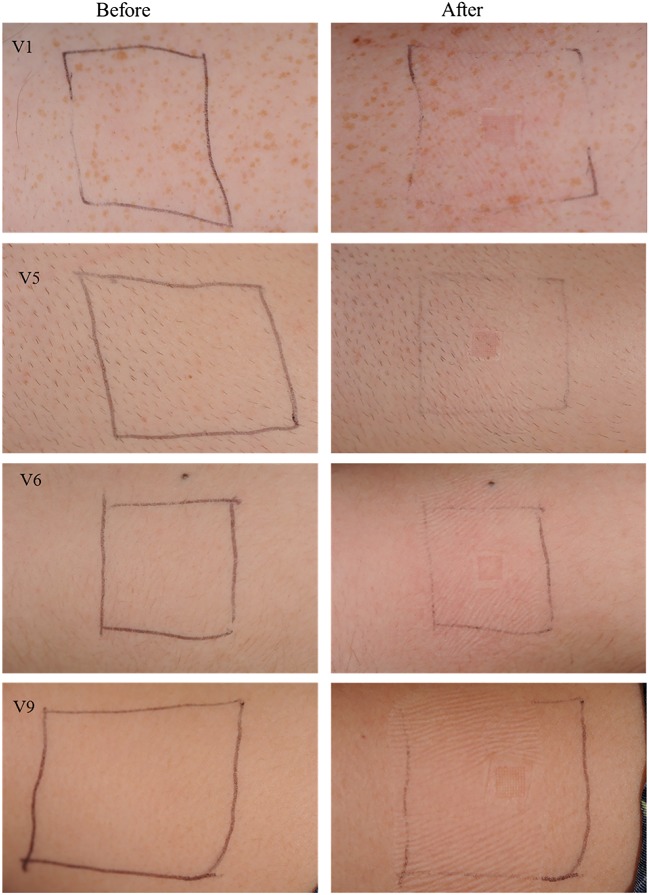
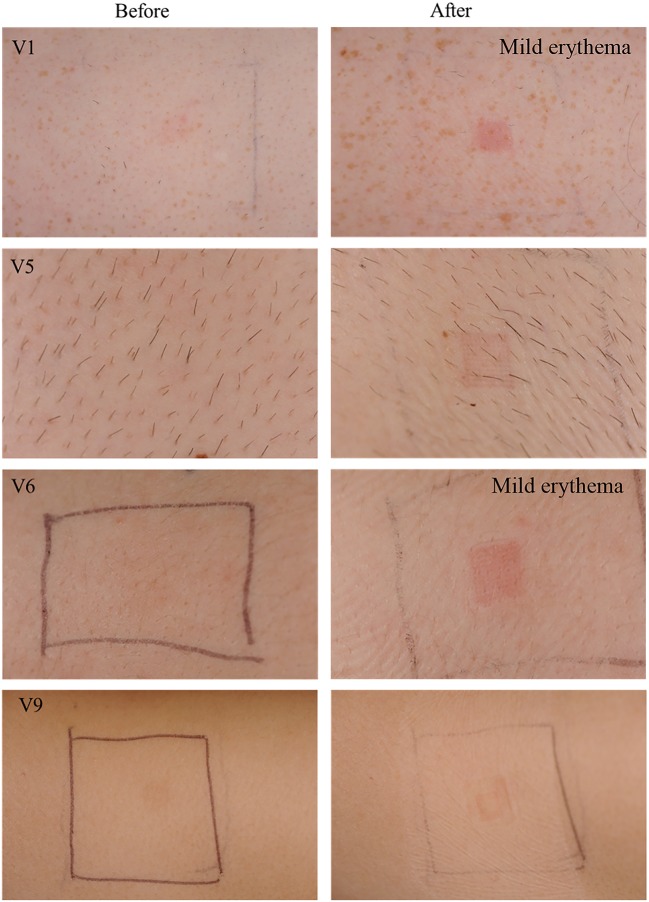
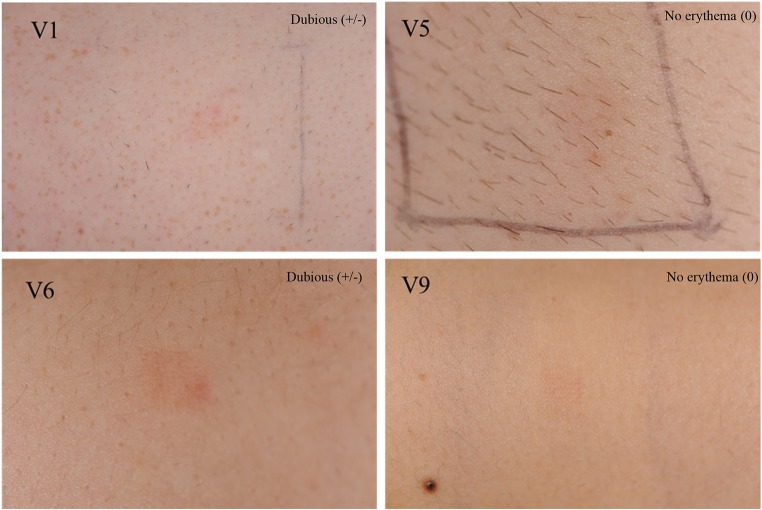
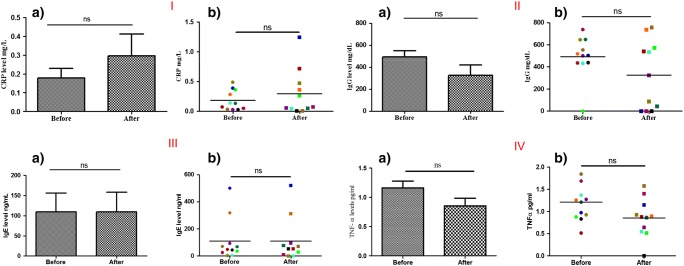
Hydrogel-forming microneedle array patches (MAPs) have been proposed as viable clinical tools for patient monitoring purposes, providing an alternative to traditional methods of sample acquisition, such as venepuncture and intradermal sampling. They are also undergoing investigation in the management of non-melanoma skin cancers. In contrast to drug or vaccine delivery, when only a small number of MAP applications would be required, hydrogel MAPs utilised for sampling purposes or for tumour eradication would necessitate regular, repeat applications. Therefore, the current study was designed to address one of the key translational aspects of MAP development, namely patient safety. We demonstrate, for the first time in human volunteers, that repeat MAP application and wear does not lead to prolonged skin reactions or prolonged disruption of skin barrier function. Importantly, concentrations of specific systemic biomarkers of inflammation (C-reactive protein (CRP); tumour necrosis factor-α (TNF-α)); infection (interleukin-1β (IL-1β); allergy (immunoglobulin E (IgE)) and immunity (immunoglobulin G (IgG)) were all recorded over the course of this fixed study period. No biomarker concentrations above the normal, documented adult ranges were recorded over the course of the study, indicating that no systemic reactions had been initiated in volunteers. Building upon the results of this study, which serve to highlight the safety of our hydrogel MAP, we are actively working towards CE marking of our MAP technology as a medical device.
Keywords: Biomarkers; Clinical translation; Hydrogels; Microneedle array patches; Microneedles; Safety; Skin barrier.
Conflict of interest statement
Ryan Donnelly is an inventor of patents that have been licenced to companies developing microneedle-based products and is a paid advisor to companies developing microneedle-based products. The resulting potential conflict of interest has been disclosed and is managed by Queen’s University Belfast. The companies had no role in the design of the study, in the collection, analyses or interpretation of data, in the writing of the manuscript or in the decision to publish the results.
Figures
References
-
- Donnelly RF, McCrudden MTC, Zaid-Alkilani A, Larraňeta E, McAlister E, Thakur RRS, McCarthy HO, Kett VL, Woolfson AD. Hydrogel-forming microneedles prepared from “super swelling” polymers enhance transdermal drug and protein delivery when combined with lyophilised wafers. PLOS One. 2014;9(10):e111547. - PMC - PubMed
-
- Leboulanger B, Guy RH, Delgado-Charro MB. Reverse iontophoresis for non-invasive transdermal monitoring. Physiol Meas. 2004;25:R35–R50. - PubMed
-
- Brunner M, Derendorf H. Clinical microdialysis: current applications and potential use in drug development. Trends Anal Chem. 2006;25(7):674–680.
-
- Caffarel-Salvador E, Brady AJ, Eltayib A, Meng T, Alonso-Vicentre A, Gonzalez-Vazquez P, Torrisi BM, Vicente-Perez EM, Mooney K, Jones DS, Bell SEJ, McCoy CP, McCarthy HO, McElnay JC, Donnelly RF. Hydrogel-forming microneedle arrays allow detection of drugs and glucose in vivo: potential for use in diagnosis and therapeutic drug monitoring. PLoS One. 2005;10(12):e0145644. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
